Oxygen tubing connectors are small plastic fittings that join two lengths of oxygen tubing so air keeps moving from your concentrator or tank to your nose. They sound minor. In daily use they decide whether your tubing trails neatly behind you or knots, kinks, and tugs at your cannula every time you turn. This guide covers the main types, how to pick one that fits, how to keep connections secure and clean, and the fire precautions that matter most when oxygen is in the home.
What a connector actually does
A connector is a short, rigid coupler with a ribbed, barbed end on each side. You push a length of tubing onto each barb, and the ridges grip it so it does not slip off. That lets you join two pieces of tubing into a longer run, or attach your nasal cannula to longer supply tubing. Most home oxygen tubing uses a standard end of about 5 to 7 mm, so most connectors fit most tubing. A good joint is snug and leak-free. A loose or cracked one lets oxygen escape, which can quietly lower the dose reaching your lungs [TGA, 2026].
The main types of oxygen tubing connectors
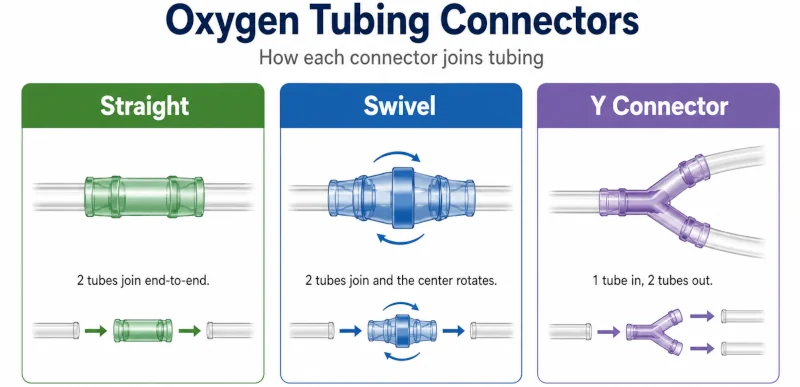
Three connectors cover almost everything a home user needs. The right one depends on how you move around and what your clinician has set up.
| Type | What it does | Best for | Keep in mind |
| Straight (in-line) | Joins two tubes end to end in a straight line. | Extending your reach simply and cheaply. | Does not rotate, so the tubing can still twist. |
| Swivel | Rotates a full turn (360°) where the two tubes meet. | Cutting down on kinks and tangles as you walk around. | Costs a little more; one extra joint to check. |
| Y-connector | Splits one line into two, or combines two oxygen sources into one. | Specific setups, such as a higher combined flow, on a clinician’s advice. | Not for everyday extending; use only if your provider recommends it. |
If your tubing twists every time you turn in a chair or pivot at the stove, a swivel is usually the upgrade worth making. The 2005 tubing study that joined lengths with swivel adapters is part of why they are a standard fix for twisting [Chron Respir Dis, 2005]. A plain straight connector is fine if you mostly need a little more length and your tubing already lays flat.
Matching a connector to your tubing
Size comes first. Standard ends are about 5 to 7 mm, and most connectors are built for that range. Some home tubing is narrow-bore (closer to 2 mm), and a standard connector will not grip it, so match the size before you buy. Material matters if your skin reacts: most connectors are rigid medical plastic such as polypropylene, and latex-free options exist for sensitive skin or a latex allergy.
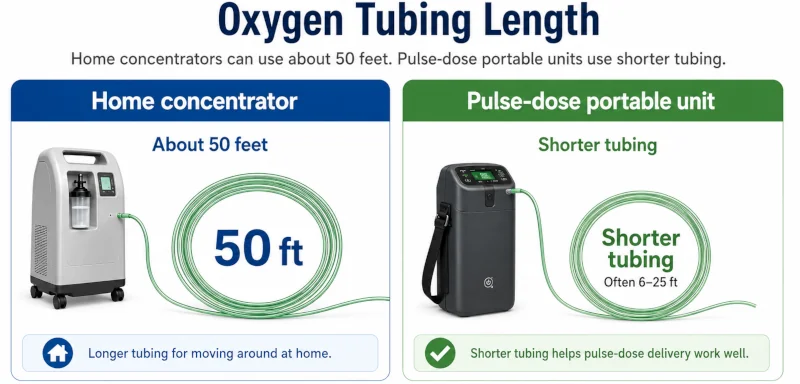
How your oxygen is delivered changes the math. Portable oxygen concentrators that pulse oxygen on each breath rely on sensing when you inhale. Long extra tubing and extra joints can blunt that signal, so keep portable setups short — a 7-foot cannula is usually enough. Continuous-flow home concentrators give you more room to add length.
Connectors, tubing length, kinks, and trips
The old rule of thumb is to keep total tubing to about 50 feet (15 m) on a home concentrator. That figure came from older cylinder-and-regulator systems, which lose pressure over long runs. When researchers added tubing in 25-foot steps up to 200 feet, concentrators and liquid-oxygen systems held their flow far better than cylinders, and the cylinder-regulator setup lost the most. They noted some concentrators can run longer lengths at low flows, but said the delivered flow should always be checked against the manufacturer’s specifications [Chron Respir Dis, 2005].
The practical takeaway: follow your equipment’s manual, and if you add length, ask your supplier to confirm you are still getting your prescribed flow at the cannula. The bigger everyday risk of long tubing is not flow — it is tripping and tangling. Tubing pooled on the floor is a common fall hazard. Swivel connectors, coiling the slack, a tubing reel, and running the line along walls all help.
Using your connectors safely
Push the tubing fully onto the barb until it seats, then give it a gentle tug to confirm it holds. A joint that pops off or hisses is leaking, and a poor connection between tubing and an outlet is a known cause of accidental disconnection [TGA, 2026].
- Inspect joints for cracks, stiffening, or yellowing, and replace any worn connector rather than nursing it along.
- Clean tubing and connectors with mild soap and warm water, rinse, and let them air-dry, following the manufacturer’s instructions. Clean parts lower the chance of breathing in germs from grimy tubing.
- Replace the nasal cannula and tubing on your supplier’s schedule — often a fresh cannula every couple of weeks and supply tubing every few months.

Fire safety matters more than any connector
Oxygen itself does not burn, but it makes other things catch fire faster and burn hotter. In a room where oxygen is flowing, clothing, bedding, hair, furniture — even the tubing and cannula — can ignite more easily than usual [Montgomery County Fire & Rescue]. The same is true of e-cigarettes, which safety bodies consider unsafe around home oxygen [ERS, 2015].
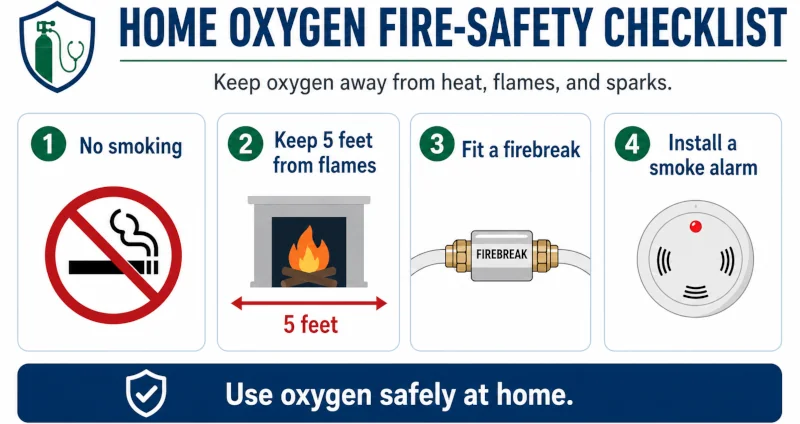
The single most important rule is no smoking, by anyone, anywhere oxygen is used or stored. Most home-oxygen burns are linked to lit cigarettes. In the United States, home fires involving oxygen equipment cause roughly 70 deaths and more than 1,000 emergency-room burn injuries each year [COPD Foundation, 2018], and about one in four reported home medical-oxygen fires is fatal [Mayo Clin Proc, 2016]. Tobacco smoke also shortens the life of oxygen equipment [ERS, 2024].
A few habits cover most of the risk:
- Keep the tubing, concentrator, and any cylinders well away from open flames and high heat — gas stoves, candles, fireplaces, space heaters, and lighters. Fire-safety agencies advise a clearance of at least five feet from any flame [COPD Foundation, 2018].
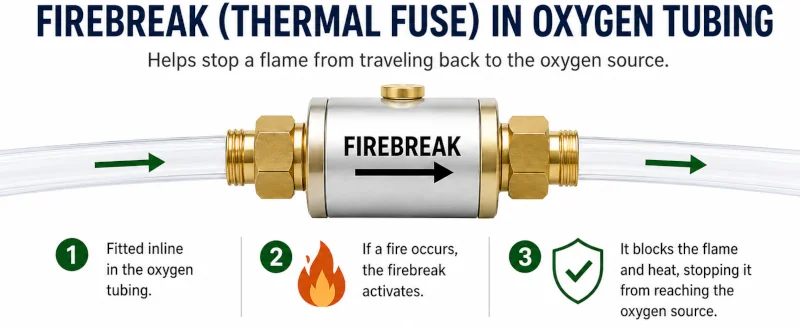
- Ask your supplier about a firebreak, also called a thermal fuse or fire-stop valve — a small device fitted into the tubing that snuffs out a flame before it can travel back along the line [COPD Foundation, 2018]. Many newer setups already include one.
- Skip oil, grease, and petroleum-based products such as petroleum jelly on your face and hands; use water-based products instead.
- Put a working smoke alarm in the room and plan how you would get out in a fire.
Where to get connectors — and what to avoid
Connectors come from durable medical equipment (DME) suppliers, pharmacies, and online retailers, and your oxygen provider can point you to ones that match your tubing. If you are still comparing equipment, our oxygen equipment reviews walk through common setups. Many plans, including Medicare and Medicaid, cover oxygen supplies as durable medical equipment, so check your specific coverage with your supplier or insurer.
Do not improvise. Hardware-store fittings, tape, and homemade adapters can leak, cut your dose, or add fire risk near an oxygen source. Use connectors made for medical oxygen, full stop.
What connectors can and cannot do
Connectors fix mechanical headaches — kinks, tangles, and reach. They will not change how much oxygen you need, treat the lung condition behind your therapy, or make up for a wrong flow setting or a failing machine. If you are short of breath despite a correct setup, the connector is not the problem.
When to call your provider — and when it is urgent
Call your supplier or provider for leaks you cannot fix by reseating the connector, tubing that keeps kinking, or skin irritation from the cannula. Do not raise your flow rate on your own: for some people, especially those with respiratory conditions such as COPD, too much oxygen can let carbon dioxide build up and become dangerous. Your prescription is set for a reason [Cleveland Clinic, 2025].
Seek urgent help — call emergency services — if you notice any of these:
- Sudden or worsening breathlessness that oxygen is not relieving, or chest pain.
- A blue tinge to the lips or fingertips, new confusion, or unusual drowsiness.
- A pulse-oximeter reading well below your usual target. These can mean too little oxygen is reaching your body.
| Health Disclaimer This article is for general education only and is not a substitute for professional medical advice, diagnosis, or treatment. Oxygen therapy is prescribed and adjusted by a licensed healthcare provider. Always follow your prescription and your equipment’s instructions, and talk with your provider or oxygen supplier before changing your tubing, connectors, flow rate, or routine. If you have a medical emergency, call your local emergency number. |
Frequently asked questions
Are all oxygen tubing connectors the same size?
Most fit standard 5 to 7 mm ends, so they are broadly compatible. Narrow-bore tubing needs a matching connector, so check the size before buying.
Do swivel connectors reduce oxygen flow?
A correctly fitted swivel does not meaningfully cut flow at home oxygen rates; its job is to stop the tubing twisting. Replace it if it cracks or starts to leak.
How long can my oxygen tubing be?
Around 50 feet is the usual guideline for home concentrators. Some go longer at low flows, but confirm with your supplier and follow your device manual. Keep pulse-dose portable setups short.
How often should I replace connectors and tubing?
Replace anything cracked, stiff, or leaking right away. Otherwise follow your supplier’s schedule — often a new cannula every couple of weeks and supply tubing every few months.
Can I make my own connector?
No. Use medical-grade connectors only. Improvised parts can leak, lower your dose, or add fire risk near oxygen.
Does insurance cover oxygen connectors?
Often yes, as part of durable medical equipment through Medicare, Medicaid, or private plans. Check your specific coverage with your supplier or insurer.
References
- Edelman DA, et al. (2016). Burn Injury Associated With Home Oxygen Use in Patients With COPD. Mayo Clinic Proceedings (via NIH/PMC). → View source
- COPD Foundation (2018). Playing with Fire – Staying Safe Using Home Oxygen Therapy. → View source
- Montgomery County Fire & Rescue Service. Smoking and Home Oxygen Tip Sheet. → View source
- Murphie P, et al. (2015). Home oxygen and domestic fires. Breathe (European Respiratory Society), 11(1). → View source
- Stancliffe M, et al. (2005). Oxygen tubing lengths and output flows: implications for patient care. Chronic Respiratory Disease, 2(4):193–197. doi:10.1191/1479972305cd095oa. → View source
- Therapeutic Goods Administration, Australia (2026). Compatibility of tubing connectors and medical gas sources – safety alert. → View source
- Cleveland Clinic (2025). Nasal Cannula: Oxygen, Flow Rate, Benefits & How To Use. → View source
- Tanash H, et al. (2024). Smoking and home oxygen therapy: a review and consensus statement. European Respiratory Review, 33(171). → View source