The dangers of smokeless tobacco are often underestimated because there is no smoke, no second-hand cloud, and no obvious cough. But the scientific evidence is consistent and, in several areas, very strong: chewing tobacco, moist snuff, dry snuff, snus, and dissolvable tobacco all deliver nicotine and known carcinogens directly into the body, and all carry real health risks. Products like Skoal and Copenhagen are not a safe alternative to cigarettes — that warning is required by U.S. law on every tin and pouch ([FDA, 2024]).
This guide explains what smokeless tobacco is, how it affects the mouth, heart, and cancer risk, who is most at risk, and — most importantly — how people actually manage to quit. Where the science is strong, we say so. Where it is mixed or limited, we say that too.
Key facts at a glance
- About 5.2 million U.S. adults currently use smokeless tobacco, roughly 2.1% of people aged 18+, and about 4.2% of men ([CDC, 2024]).
- Smokeless tobacco causes cancers of the mouth, esophagus, and pancreas — a conclusion reached by the International Agency for Research on Cancer ([IARC, 2007]).
- It contains at least 28 known or probable human carcinogens, with tobacco-specific nitrosamines (TSNAs) as the most studied ([NCI, 2023]).
- Nicotine exposure from a can of dip can match or exceed that of 60 cigarettes, which is why addiction sets in quickly ([NIDA, 2021]).
- Every package must carry the warning: “This product is not a safe alternative to cigarettes.” [FDA, 2024]
What is smokeless tobacco?
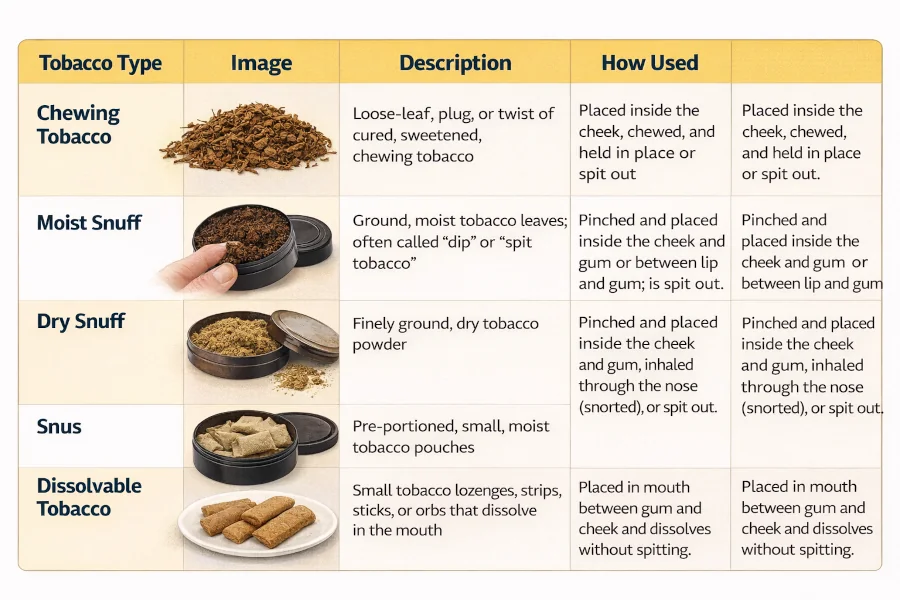
Smokeless tobacco is any tobacco product used in the mouth or nose instead of being burned and inhaled. The two best-known forms in the United States are chewing tobacco and snuff, but the category also includes snus and dissolvable tobacco. All of them work the same basic way: tobacco leaf sits against the lining of the mouth, nicotine and other chemicals are absorbed through the tissue, and the user spits out the juice or swallows it.
The table below summarises the main product types you will see on U.S. shelves. Even “low-nitrosamine” products like some Swedish-style snus still deliver high doses of nicotine and have not been shown to be risk-free ([NCI, 2023]).
| Product type | How it is used | Examples | Key concern |
| Moist snuff / dip | Pinch placed between lip or cheek and gum | Skoal, Copenhagen, Grizzly | High nicotine delivery; oral lesions |
| Dry snuff | Powdered tobacco, sometimes sniffed or placed in mouth | Traditional dry snuffs | Nasal and oral cancer risk |
| Loose-leaf chewing tobacco | Shredded leaf chewed as a “quid” | Red Man, Levi Garrett | Gum recession, tooth decay, oral cancer |
| Plug / twist | Compressed cake or rope of cured leaf | Days Work, Cannon Ball | Same cancer and nicotine risks |
| Snus | Small pouch placed under the upper lip; not spit | General, Camel Snus | Addiction; lower but not zero cancer risk |
| Dissolvable tobacco | Lozenges, strips, or sticks that dissolve in the mouth | Camel Orbs, Sticks, Strips | Child poisoning risk; addiction |
Is smokeless tobacco safer than cigarettes?
This is the single most common question, and it deserves a careful answer. Smokeless tobacco does not produce the tar and carbon monoxide generated when tobacco is burned, so lung cancer and chronic obstructive pulmonary disease are less tightly linked to it than to cigarettes. That is a real difference.
But “less harmful in some ways” is not the same as “safe.” Public health authorities are clear that switching from cigarettes to dip or chew is not a proven path to quitting, and long-term smokeless tobacco users still face elevated risks of several cancers, heart attack, and stroke ([American Heart Association, 2023]; [U.S. Surgeon General, 2014]). The FDA requires a warning label specifically saying the product is not a safe alternative to cigarettes because the evidence to support such a claim does not exist.
The main dangers of smokeless tobacco
1. Cancer of the mouth, esophagus, and pancreas
The International Agency for Research on Cancer classifies smokeless tobacco as a Group 1 carcinogen — the same category as asbestos and cigarette smoke — meaning there is sufficient evidence that it causes cancer in humans ([IARC, 2012]). The cancers most consistently linked to smokeless tobacco are:
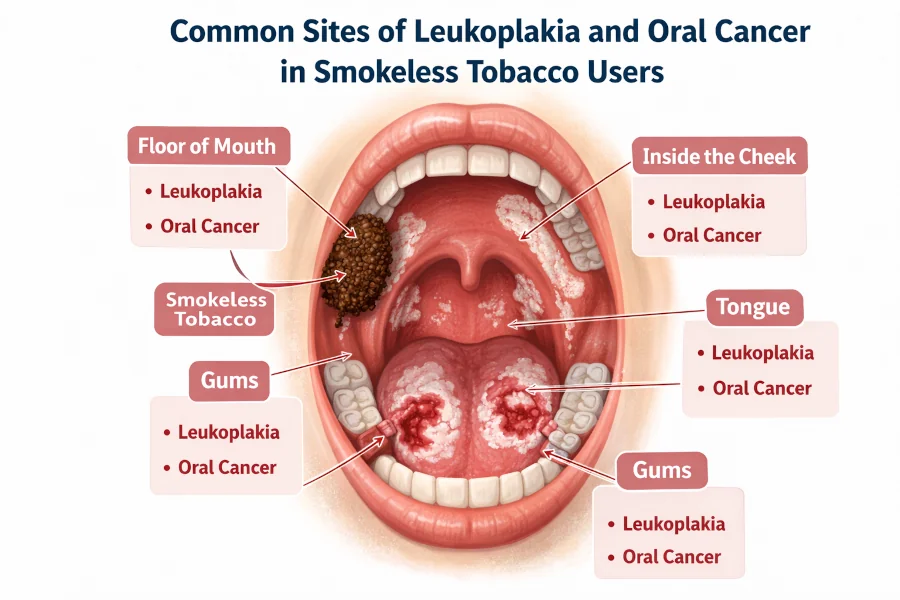
- Oral cancer — lips, tongue, cheek, gums, floor of the mouth, and hard palate.
- Esophageal cancer — especially among long-term daily users.
- Pancreatic cancer — the evidence is weaker than for oral cancer, but several large cohort studies have found a statistically significant increase in risk.
The main chemical culprits are tobacco-specific N-nitrosamines (TSNAs) such as NNN and NNK, which form during the curing and fermentation of tobacco leaf. These compounds damage DNA in ways that are biologically plausible causes of cancer ([NCI, 2023]).
A visible early warning is leukoplakia, a white, thickened patch that forms where the quid sits. Most cases are not cancer, but a small percentage will progress, which is why any white patch that does not go away within two weeks after stopping the product should be checked by a dentist or doctor ([Mayo Clinic, 2023]).
2. Nicotine addiction
Nicotine is absorbed directly through the lining of the mouth, and the dose from smokeless tobacco is high and sustained. The National Institute on Drug Abuse notes that holding an average-size dip in the mouth for about 30 minutes can deliver as much nicotine as smoking about three cigarettes, and a typical can’s worth of dip can match a pack or more ([NIDA, 2021]).
Addiction is not a character flaw — it is a predictable response to a drug that physically rewires reward pathways. This matters because most people who try to quit cold turkey fail on the first attempt, and that failure can feel personal when it is actually pharmacological.
3. Heart attack and stroke
Nicotine raises heart rate and blood pressure, stiffens arteries, and promotes the cellular changes that lead to atherosclerosis. A pooled analysis of European and American cohort studies found that smokeless tobacco use was associated with an increased risk of fatal heart attack and fatal stroke, though the increase was smaller than for cigarette smoking ([Boffetta & Straif, BMJ 2009]). The American Heart Association warns that smokeless tobacco is not a heart-safe alternative to cigarettes.
4. Gum disease, tooth loss, and oral damage
The abrasive texture and sugars in many smokeless products drive up plaque formation and tooth decay, especially where the quid is held. Over time this leads to:
- Receding gums at the site of the dip, often exposing tooth roots.
- Staining of the teeth and bad breath.
- Bone loss around the teeth and, eventually, loose or lost teeth.
- Chronic mouth sores that may be painless in the early stages.
The FDA requires every smokeless tobacco package to carry a warning that the product “can cause gum disease and tooth loss.” That is not marketing caution — it is the distilled conclusion of decades of dental research ([FDA, 2024]).
5. Pregnancy and reproductive risks
Nicotine crosses the placenta. Studies from South Asia, where smokeless tobacco use in pregnancy is more common, show associations with stillbirth, preterm birth, and low birth weight ([Inamdar et al., Nicotine & Tobacco Research 2015]). Pregnant women should not use any form of tobacco.
What the evidence actually supports
It is worth being precise about how strong the science is for different claims, because honest communication is more persuasive than exaggeration.
| Health effect | Strength of evidence | What it means |
| Oral cancer | Strong | Consistent across dozens of studies and confirmed by IARC. |
| Esophageal cancer | Strong | Supported by large cohort studies and IARC classification. |
| Pancreatic cancer | Moderate | Multiple studies show an increased risk; effect size varies. |
| Nicotine addiction | Strong | Well-established pharmacology and clinical experience. |
| Fatal heart attack / stroke | Moderate | Pooled analyses show increased risk vs. non-users. |
| Gum disease, tooth loss, leukoplakia | Strong | Clinically visible and repeatedly documented. |
| Type 2 diabetes | Limited / mixed | Some evidence of higher risk; not yet conclusive. |
| Effectiveness as a quit-smoking aid | Weak | Not endorsed by U.S. guidelines; often prolongs nicotine dependence. |

Who should avoid smokeless tobacco entirely
There is no medically approved use of smokeless tobacco. Certain groups face additional risk and should avoid it without exception:
- Children and teenagers — nicotine affects the developing brain and strongly predicts lifelong dependence.
- Pregnant and breastfeeding women — nicotine crosses the placenta and passes into breast milk.
- People with heart disease, high blood pressure, or a history of stroke — nicotine acutely raises blood pressure and heart rate.
- People with diabetes — nicotine can worsen insulin resistance and blood sugar control.
- Anyone with a previous oral, head, or neck cancer — continued use sharply raises the risk of a second primary cancer.
- People using medications sensitive to nicotine — including certain asthma drugs, blood pressure medicines, and some antidepressants. Talk to a pharmacist if you are unsure.
Red-flag symptoms: when to see a doctor now
Some findings should never be ignored. If you use or have used smokeless tobacco and notice any of the following, make an appointment with a dentist, oral surgeon, or primary-care doctor within the next week or two — sooner if the symptoms are severe.
- A white, red, or speckled patch in the mouth that does not go away within 2 weeks.
- A sore, ulcer, or lump in the mouth, on the lip, or on the tongue that lasts more than 2 weeks.
- Persistent bleeding, numbness, or pain in the mouth, ear, or jaw.
- Loose teeth, pain on chewing, or a change in the way your teeth fit together.
- Difficulty swallowing, hoarseness, or a feeling that something is stuck in your throat.
- Unexplained weight loss or a lump in the neck.
Any of these symptoms warrant an in-person examination. Early-stage oral cancers are often highly treatable; advanced ones are not ([American Cancer Society, 2024]).
How to quit smokeless tobacco
Quitting is hard, but it is absolutely possible, and the health benefits begin within days. The same evidence-based methods that work for cigarettes work for dip and chew. A sensible plan combines behavioural support, medication if appropriate, and concrete habit changes. If you are also thinking about food-based support during the transition, our guide to foods that can help you quit smoking is worth a read.
Step 1: Set a quit date and tell someone
Pick a specific date within the next two weeks. Tell at least one person whose support you trust. Throw out every can, pouch, and spit cup in your house, car, and workplace the night before. The goal is to remove the option entirely for the first critical days.
Step 2: Consider FDA-approved cessation medication
Nicotine replacement therapy (patch, gum, lozenge, inhaler, nasal spray) roughly doubles the chance of quitting compared with willpower alone, and prescription medicines like varenicline and bupropion are also effective ([Cochrane Review, 2018]). These are approved for smoking cessation and are commonly used off-label for smokeless tobacco; discuss the fit with your doctor or pharmacist.
Step 3: Use a proven behavioural program
Free, evidence-based support is available by calling 1-800-QUIT-NOW, visiting smokefree.gov, and the My Last Dip program designed specifically for smokeless tobacco users. Group and phone counselling meaningfully improve success rates.
Step 4: Replace the physical habit
Much of what keeps smokeless tobacco in your pocket is ritual, not chemistry. Sugar-free gum, sunflower seeds, toothpicks, herbal (tobacco-free) chew pouches, and cold water can substitute for the hand-to-mouth action in the first weeks. Short walks after meals break the strongest cue. Exercise also reduces craving intensity.
Step 5: Protect your heart and mouth during withdrawal
The first two weeks are the hardest, and during this period your blood pressure and heart rate begin to improve almost immediately. Eating a heart-healthy diet and including foods linked with stroke prevention — vegetables, fruit, whole grains, legumes, and nuts — helps the cardiovascular system recover. Book a dental cleaning in your first smoke-free month so your dentist can establish a baseline for future oral checks.
For a more general plan, our article on how to stop smoking walks through the same steps in more detail, and most of the advice applies equally to smokeless tobacco.
Realistic expectations
Most people who quit successfully have tried more than once. Slips are common and do not mean failure — they mean your plan needs adjustment. Cravings typically peak in the first 72 hours, drop sharply after two weeks, and become occasional by week six. The sore spots and white patches in the mouth often begin to heal within two to six weeks of stopping.
Health disclaimer
| ⚠ Health Disclaimer This article is for general educational and informational purposes only. It is not medical advice and is not a substitute for diagnosis, treatment, or guidance from a qualified healthcare professional. No food, herb, supplement, or behaviour change mentioned here is intended to diagnose, treat, cure, or prevent any disease. If you use smokeless tobacco and notice a lump, white patch, persistent sore, bleeding, numbness, or difficulty chewing or swallowing, see a dentist or physician promptly. If you are pregnant, breastfeeding, have heart disease, diabetes, or any chronic condition, speak with your doctor before making changes to your tobacco use or starting any cessation medication. In the United States, free confidential help is available 24/7 at 1-800-QUIT-NOW or SmokefreeTXT. |
Frequently asked questions
Is chewing tobacco really as addictive as cigarettes?
In terms of nicotine delivered to the bloodstream, yes. Long-held dip can deliver more nicotine per session than a single cigarette, and blood nicotine levels in regular dippers are comparable to those in pack-a-day smokers. That is why people who try to quit without support have such a hard time.
Does snus cause less cancer than American dip?
Swedish-style snus is manufactured with a pasteurisation step that reduces — but does not eliminate — tobacco-specific nitrosamines. Studies from Sweden show lower oral cancer rates than older smokeless products, but the evidence for pancreatic cancer and cardiovascular events is mixed. Snus is not a harm-free option and is not approved by the FDA as a smoking cessation tool.
How long after quitting does my cancer risk drop?
Oral tissue begins healing within weeks of stopping. The risk of oral and esophageal cancer declines over years, but it does not return immediately to that of a lifelong non-user. The sooner you quit, the sooner the downward trend begins.
Can herbal or “natural” chew products help me quit?
Tobacco-free herbal chew (such as mint-based pouches) can be useful as a short-term substitute for the physical habit because it contains no nicotine. The evidence that it actually improves long-term quit rates is limited, and some products contain caffeine or other stimulants. Think of herbal chew as a training wheel, not a treatment.
Are dissolvable tobacco lozenges and strips safer?
They avoid the need to spit and are less visible, but they still deliver nicotine and tobacco-specific nitrosamines. They also pose a poisoning risk to young children, who can mistake them for candy. The American Academy of Pediatrics has warned about this specifically.
Recommended images for this article
These images are suggestions for the editor; they are not included in the document itself so the site team can produce or license originals.
- Labelled diagram of the mouth showing common dip-lesion sites. Filename: dangers-of-smokeless-tobacco-oral-lesion-sites.webp. Alt: “Labelled mouth diagram showing common sites of leukoplakia and oral cancer in smokeless tobacco users.” Placement: inside the cancer section.
- Comparison chart of product types. Filename: smokeless-tobacco-types-comparison-chart.webp. Alt: “Chart comparing chewing tobacco, moist snuff, dry snuff, snus, and dissolvable tobacco.” Placement: next to the comparison table.
- Evidence-strength infographic. Filename: smokeless-tobacco-evidence-strength-chart.webp. Alt: “Infographic showing strength of evidence linking smokeless tobacco to oral cancer, heart disease, and other conditions.” Placement: in the “What the evidence actually supports” section.
- Quit-plan timeline. Filename: how-to-quit-smokeless-tobacco-30-day-timeline.webp. Alt: “30-day timeline showing craving peaks and healing milestones after quitting smokeless tobacco.” Placement: in the “How to quit” section.
- Red-flag symptom checklist. Filename: smokeless-tobacco-oral-cancer-red-flags.webp. Alt: “Checklist of red-flag mouth symptoms that require a dental or medical visit.” Placement: in the “Red-flag symptoms” section.
References
- Centers for Disease Control and Prevention. Smokeless Tobacco Product Use in the United States. 2024. → View source
- National Cancer Institute. Smokeless Tobacco and Cancer Fact Sheet. 2023. → View source
- International Agency for Research on Cancer. Smokeless Tobacco and Some Tobacco-specific N-Nitrosamines. IARC Monograph Vol. 89. 2007. → View source
- IARC. Personal Habits and Indoor Combustions, Monograph Vol. 100E. 2012. → View source
- U.S. Food and Drug Administration. Smokeless Tobacco Product Warning Statements. 2024. → View source
- National Institute on Drug Abuse. What are the physical health consequences of tobacco use? 2021. → View source
- Boffetta P, Straif K. Use of smokeless tobacco and risk of myocardial infarction and stroke: systematic review with meta-analysis. BMJ. 2009;339:b3060. → View source
- Inamdar AS, et al. Maternal smokeless tobacco use in pregnancy and adverse health outcomes in newborns: a systematic review. Nicotine Tob Res. 2015;17(9):1058-1066. → View source
- Hartmann-Boyce J, et al. Nicotine replacement therapy versus control for smoking cessation. Cochrane Database of Systematic Reviews. 2018. → View source
- Mayo Clinic. Leukoplakia — Symptoms and causes. 2023. → View source
- American Cancer Society. Signs and Symptoms of Oral Cavity and Oropharyngeal Cancer. 2024. → View source
- American Heart Association. Is Smokeless Tobacco Safer Than Smoking? 2023. → View source
- U.S. Surgeon General. The Health Consequences of Smoking — 50 Years of Progress. 2014. → View source