If you want to know how to lose stubborn belly fat without surgery, the honest answer comes in two parts, and the first part matters far more than the devices you have probably seen advertised. Most belly fat responds to the same unglamorous habits that lower your health risk: what you eat, how you move, and how you sleep. A handful of in-clinic procedures can smooth a small, diet-resistant bulge, but they are body-contouring tools, not weight-loss treatments, and they do nothing for the deeper fat that actually affects your health. [AAD].
So if you have seen ads promising that a juice or a 7-second trick “eats through 62 pounds of fat,” treat them as marketing. They are not how fat loss works. Here is what does.
Two kinds of belly fat, and why the difference matters
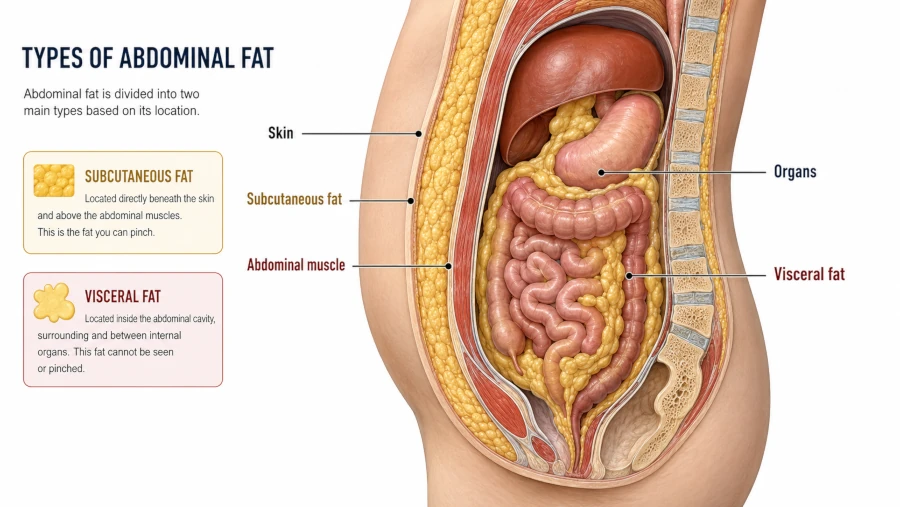
Not all belly fat is the same. About 90% of body fat is subcutaneous — the soft, pinchable layer just under the skin. The other roughly 10% is visceral fat, which sits deeper in the abdomen and wraps around the liver, intestines, and other organs. [Harvard Health, 2024] Visceral fat is the one that affects your health most. It behaves like an active organ, releasing inflammatory signals tied to higher risk of heart disease, type 2 diabetes, and other conditions. [Cleveland Clinic, 2025]
You can get a rough read at home with a tape measure. Stand, wrap it around your bare middle just above the hip bones, exhale, and read it without sucking in. A waist over 35 inches in women or 40 inches in men signals an unhealthy amount of belly fat and a higher risk of problems. [Mayo Clinic Press, 2026]
| Subcutaneous fat | Visceral fat | |
| Where it is | Just under the skin; the part you can pinch | Deep in the belly, around internal organs |
| Share of body fat | About 90% | About 10% |
| Health impact | Mostly cosmetic until present in large amounts | Drives inflammation; linked to heart disease and diabetes |
| Responds to | Diet and exercise (the surface pocket can be slow to shift) | Diet and exercise — and it often shrinks first |

Why you can’t “target” belly fat
Spot reduction is a myth. Crunches and planks strengthen the muscle underneath, but they do not burn the fat sitting on top of it. [Harvard Health, 2024] Fat loss is whole-body: as your overall fat drops, it leaves the belly too, but you cannot dictate the order. Where it goes first is set largely by genes, sex, and hormones.
There is a silver lining. Because visceral fat is metabolically active, it tends to respond early to diet and exercise — sometimes faster than the stubborn surface fat you can actually see. [Mayo Clinic, 2024]
What actually works to lose stubborn belly fat without surgery

The foundation is a modest, sustainable calorie deficit paired with movement you will keep doing. Nothing here is exotic, and that is the point — the boring version is the one that works.
Move your body, two ways
Aim for at least 150 minutes a week of moderate aerobic activity — brisk walking, cycling, swimming — and add strength training two or three days a week. Even when the scale barely moves, exercise trims visceral fat and builds muscle. [Harvard Health, 2024] [Mayo Clinic, 2024]
Eat in a way you can keep up
Focus on portion control and minimally processed foods: vegetables, whole grains, fruit, nuts, and lean protein, with plenty of fiber. Cut back on sugary drinks and ultra-processed snacks, and watch fructose-sweetened beverages in particular. [Mayo Clinic Press, 2026] For practical ideas, see foods that support weight loss and a simple approach to cutting back on added sugar. Be skeptical of “fat-burning” herbs sometimes promoted for metabolism — they are no substitute for the basics.
Sleep, stress, and alcohol
These get ignored, and they shouldn’t. Short sleep is linked to more visceral fat gain in younger adults, ongoing stress keeps cortisol elevated, and heavy drinking tracks with a larger waist. [Harvard Health, 2024] Most adults do best with 7 to 9 hours of sleep.
A realistic pace: with a deficit of roughly 300 to 500 calories a day plus regular exercise, about half a pound to a pound of body fat per week is typical, and many people notice a smaller waist within 4 to 8 weeks. The bathroom scale can mislead here — track the tape measure and how your clothes fit instead. [Mayo Clinic, 2024]
Non-surgical procedures: what they can and can’t do
Sometimes a small pocket of fat won’t budge even at a stable, healthy weight. That narrow situation is what in-clinic, non-surgical treatments are built for. Dermatology and plastic-surgery bodies are clear about the right candidate: someone at or near their goal weight with a small bulge that resists diet and exercise — not someone trying to lose a lot of weight. [AAD] None of these treatments reduce visceral fat or improve metabolic health. [ASPS]
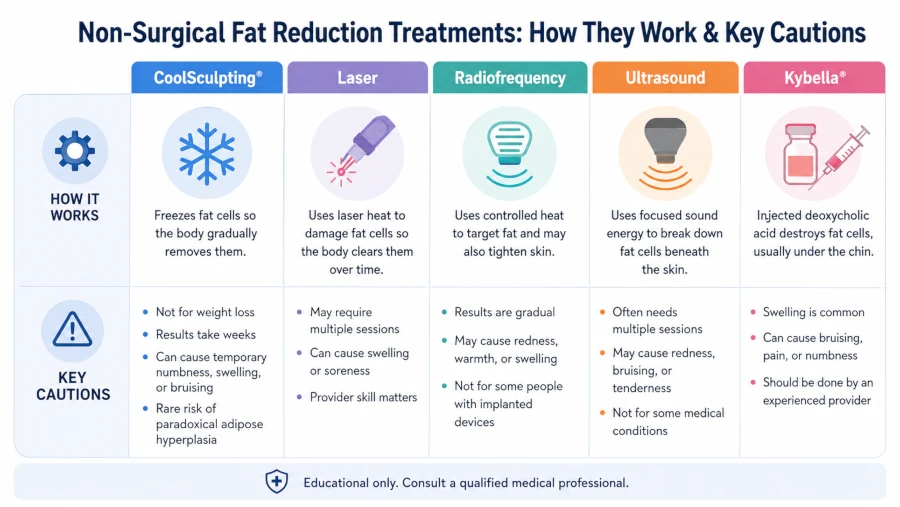
| Treatment | How it works / realistic result | Worth knowing |
| Cryolipolysis (CoolSculpting) | Controlled cooling kills fat cells in a suctioned area; ~15–28% of the fat layer there, cleared over weeks to months | Does not change body weight; small risk of paradoxical adipose hyperplasia (a firm fat lump that needs surgery to fix) |
| Laser (e.g., SculpSure) | Heat damages fat cells; gradual contouring over ~6–12 weeks, often several sessions | FDA-cleared for abdomen and flanks; temporary soreness and swelling |
| Radiofrequency | Heat targets fat and can tighten skin; modest, gradual results | Avoid with implanted devices such as pacemakers in the treated area |
| Ultrasound | Sound waves break down fat-cell walls; small circumference changes | Spa “cavitation” has weaker, shorter-lived evidence; manage expectations |
| Injectable deoxycholic acid (Kybella) | Injection dissolves fat cells | FDA-approved only for fat under the chin — not the belly |
| Red light / low-level laser | Light prompts fat cells to release their contents; subtle effect | Evidence is limited; results tend to be small and temporary |
Cryolipolysis (CoolSculpting)

Controlled cooling kills some fat cells in a suctioned area, and the body clears them over the following months. Reviews put the fat-layer reduction in a treated area at roughly 15 to 28% by caliper measurement. [Ingargiola et al., 2015] But a 2025 meta-analysis found it lowers local fat thickness and circumference without changing body weight — useful for shaping, not for slimming down overall. [WJPS, 2025]
The complication worth understanding is paradoxical adipose hyperplasia (PAH): months after treatment, the treated area grows a firm, painless mass of fat instead of shrinking. The manufacturer once estimated this near 1 in 4,000 treatments, but independent case series have reported it far more often — roughly 0.5% to 2% — and it appears more common in men. [StatPearls, 2024] PAH does not resolve on its own; correcting it usually means liposuction or surgery, which defeats the reason most people chose a non-surgical option. [Keaney & Gold, 2016]
Laser and radiofrequency
Devices such as SculpSure (laser) and various radiofrequency systems use heat to damage fat cells. They are cleared for areas like the abdomen and flanks, results build gradually over several weeks, and most people need more than one session. Side effects are usually limited to temporary soreness, redness, or swelling. As with cooling, the changes are subtle. [AAD]
Injectable deoxycholic acid (Kybella)
This is where the original advice circulating online gets it wrong. Kybella is FDA-approved only for fat below the chin (submental fat). The FDA states plainly that its safety and effectiveness outside the chin area have not been established, so using it on the belly is off-label. [FDA, 2022] Expect noticeable swelling for a few days after treatment; rare nerve injury can temporarily affect the smile.
Ultrasound and red light therapy
“Cavitation” ultrasound and low-level light treatments are heavily marketed, often at spas, but the evidence behind them is thinner. Circumference changes tend to be small and may not last. If you try them, keep your expectations modest and your budget modest to match. [AAD]
Safety, side effects, and who should skip these treatments
In trained hands, non-surgical fat reduction is generally low-risk. The common side effects are temporary: redness, swelling, bruising, tenderness, and numbness for days to a few weeks. [AAD] Still, these procedures are not for everyone.
Use caution or avoid them if you:
- Are pregnant or breastfeeding.
- Have a cold-sensitivity disorder such as Raynaud’s, cold urticaria, or cryoglobulinemia — these rule out cryolipolysis specifically.
- Have a pacemaker or metal implant near the area you’d treat (a concern for energy-based devices).
- Are hoping to treat obesity or lower visceral fat — these are the wrong tools for that job.
Choose a board-certified dermatologist or plastic surgeon, and be wary of bargain “cavitation” packages at unlicensed spas. A good provider will tell you honestly whether you are a candidate — and may say no. [ASPS]
When belly fat needs a doctor, not a device
Some situations call for medical advice rather than a cosmetic fix:
- A waist above the risk thresholds (35 inches for women, 40 for men) along with high blood pressure, high blood sugar, or abnormal cholesterol — that is a health conversation, not a contouring one.
- Rapid or unexplained weight change in either direction, which can signal an underlying condition.
- Belly fat that won’t shift despite consistent, sustained effort — a clinician can discuss medical weight-management options, including prescription medications and, for some people, bariatric surgery.
If diet and exercise have not been enough, that is information, not failure. A primary care clinician is the right next stop. [Mayo Clinic, 2024]
| Health Disclaimer This article is for general education only and is not medical advice. It cannot account for your personal health, medications, or history. Before starting a weight-loss plan or booking any cosmetic procedure, talk with a qualified healthcare professional. No food, drink, supplement, or device “melts” or “eats through” belly fat, and results from any approach vary from person to person. If you have a medical condition or take prescription medication, get individual guidance before making changes. |
Frequently Asked Questions
Can you really lose belly fat without surgery?
Yes. Most belly fat — especially the deeper visceral fat that affects your health — responds to diet, regular activity, and better sleep. Non-surgical procedures only smooth small surface bulges; they are not how you lose meaningful fat.
Does CoolSculpting get rid of belly fat for good?
It permanently removes some fat cells in the treated area, but the cells that remain can still enlarge if you gain weight, and it does not lower your overall weight or visceral fat. It also carries a small risk of paradoxical adipose hyperplasia.
Is there a juice, tea, or pill that melts belly fat?
No. Claims like “lose 62 pounds with a fizzy juice” are advertising, not medicine. There is no drink or supplement that selectively burns belly fat.
How fast will I see results from lifestyle changes?
With a modest calorie deficit and regular exercise, many people notice a smaller waist within 4 to 8 weeks. Visceral fat often responds first, even before the scale moves much.
Are non-surgical fat treatments safe?
For the right candidate and a trained provider, they are generally low-risk, with temporary swelling, bruising, or numbness. Cryolipolysis carries the uncommon PAH risk, and these treatments are not advised during pregnancy or for people with cold-sensitivity disorders.
Can I lose fat from just my belly?
No. Spot reduction isn’t possible — you lose fat from the whole body as your total fat drops, and genetics largely decide the order.
References
- Harvard Health Publishing. “Taking aim at belly fat.” Reviewed 2024. → View source
- Cleveland Clinic. “Visceral fat vs. subcutaneous fat.” 2025. → View source
- Mayo Clinic. “Belly fat in men: Why weight loss matters.” → View source
- Mayo Clinic. “Belly fat in women: Taking — and keeping — it off.” → View source
- Mayo Clinic Press. “The truth about belly fat.” 2026. → View source
- American Academy of Dermatology. “Non-invasive fat removal: What can you expect?” → View source
- American Society of Plastic Surgeons. “Nonsurgical fat reduction.” → View source
- Ingargiola MJ, et al. “Cryolipolysis for fat reduction and body contouring: safety and efficacy of current treatment paradigms.” Plast Reconstr Surg. 2015;135(6):1581-90. → View source
- Effectiveness of cryolipolysis in body contouring and fat reduction: a systematic review and meta-analysis. World J Plast Surg. 2025 (PubMed). → View source
- Kelly E, Rodriguez-Feliz J. “Paradoxical Adipose Hyperplasia.” StatPearls, NCBI Bookshelf. 2024. → View source
- Keaney TC, Gold MH. “Men at risk for paradoxical adipose hyperplasia after cryolipolysis.” J Cosmet Dermatol. 2016 (PubMed). → View source
- U.S. FDA. KYBELLA (deoxycholic acid) prescribing information. 2022. → View source