The best time to check blood pressure is not a single fixed moment — it depends on what question you are trying to answer. Morning readings reveal how your cardiovascular system behaves during its most vulnerable daily window.
Evening readings capture the cumulative effect of the day behind you. For most people starting home monitoring, both windows are necessary for at least a week to establish a meaningful baseline. After that, one consistent time is usually enough for routine tracking.
Most people treat blood pressure like a fixed number — something that should stay put if you are healthy. It does not work that way. Blood pressure shifts in response to your nervous system, hormones, physical activity, stress, meals, hydration, and dozens of other variables across the day. A 20-point swing between morning and evening is not a malfunction. It is your body doing what bodies do.
The practical question is which time gives you useful data. This article walks through what morning and evening readings each tell you, the most common timing mistakes that distort results, and a step-by-step protocol drawn from the AHA/AMA Joint Policy Statement on Home Blood Pressure Monitoring. [Shimbo et al., 2020]
⚠ MEDICAL DISCLAIMER This article on the best time to check blood pressure is for educational purposes only and is not a substitute for medical advice. If you have high blood pressure, heart disease, kidney disease, are pregnant, or take prescription medications, consult a qualified clinician before changing treatment, diet, exercise, or supplements. Do not stop or adjust blood pressure medication without your prescriber’s guidance.
Why Your Blood Pressure Changes Throughout the Day
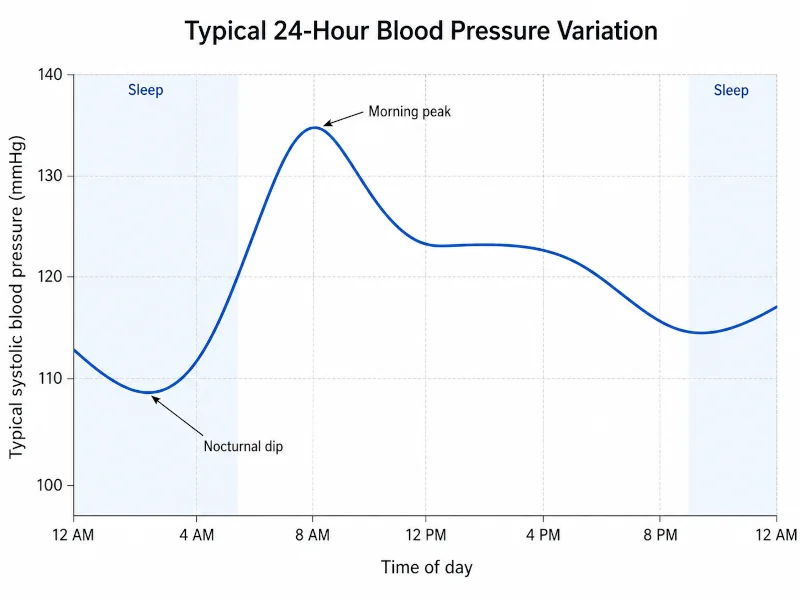
Blood pressure is not a static value. It follows a predictable daily rhythm — rising sharply in the early morning, remaining elevated through midday, easing through the afternoon, and falling to its lowest point during deep sleep. This cycle is driven by the autonomic nervous system, circadian hormones, physical activity, sodium intake, and hydration.
During the early morning hours, the body releases cortisol and adrenaline to prepare for the demands of the day — a well-documented hormonal pattern tied to the hypothalamic-pituitary-adrenal axis and its circadian rhythm. [Nakamura et al., 2021] Blood vessels constrict and heart rate rises in response, producing the well-known morning blood pressure surge.
Understanding this rhythm matters for two reasons: first, the time of your reading determines what you are actually measuring; second, disruptions to the normal pattern — such as blood pressure that remains elevated overnight — carry their own clinical significance. [Gavriilaki et al., 2020]
Morning vs. Evening: What Each Measurement Actually Captures
Morning readings
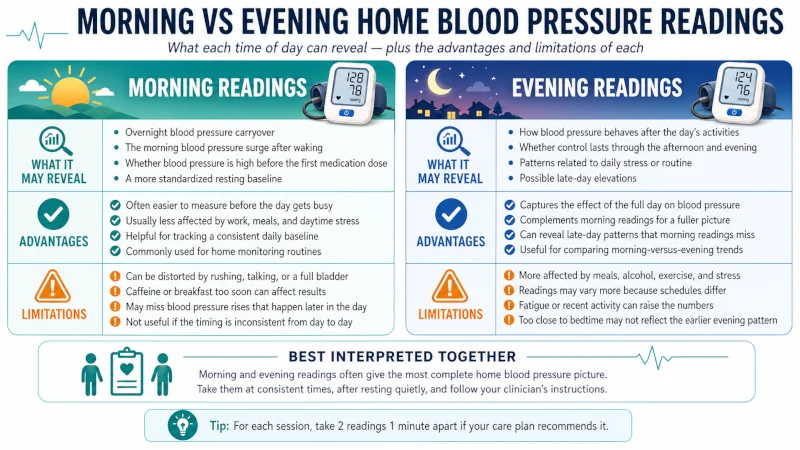
Between roughly 6 a.m. and noon, the cortisol and adrenaline surge that wakes the body also drives blood pressure up — often by 10 to 30 mmHg above overnight levels. Research has linked exaggerated morning surges to increased stroke risk in some populations. [Kario, 2010]
Morning readings also expose medication gaps. If you take blood pressure medication in the evening, its effects may be waning by 7 a.m. Your first measurement of the day shows your cardiovascular system at or near its pharmacological trough — the most vulnerable window of your treatment cycle. [Kario, 2010] For a step-by-step technique guide regardless of timing, see our how to take blood pressure at home.
Evening readings
Evening readings capture the day’s accumulated effects: dietary sodium, stress, physical exertion, dehydration, and fatigue. If you take blood pressure medication in the morning, your evening reading shows whether coverage is still effective 10 to 12 hours later.
Evening readings typically run 5 to 15 mmHg lower than morning readings in people with well-controlled blood pressure. Consistently higher evening readings, or an unusually large gap between morning and evening, are patterns worth discussing with a clinician.
Neither time is inherently more accurate. They are measuring different physiological states. The goal is to understand what each tells you, use that information together, and track the right time consistently.
What You Can Learn from Comparing Both Times
| Time | What it reveals | Advantages | Limitations |
| Morning (within 1 hr of waking; before meds, coffee, or breakfast) | Medication trough, morning surge, overnight cardiovascular status | Consistent conditions; catches high-risk window; strongest predictor of cardiovascular events in research | May appear elevated vs all-day average; easy to rush prep steps |
| Evening (before bed; at least 1 hr after eating, exercise, or alcohol) | Medication efficacy at trough; daily stress load; diet and activity effects | Reflects real-world conditions; often lower; easy to anchor to a bedtime routine | More variable; easy to skip after a tiring day |
The American Heart Association recommends checking blood pressure at both morning and evening time points for at least three to seven days when starting home monitoring, using a standardised protocol each time. [Shimbo et al., 2020]
For more on device selection and positioning, see our guide to home blood pressure monitoring.
Five Common Timing Mistakes That Distort Your Readings
Mistake 1: Comparing a morning reading to yesterday’s evening reading. Blood pressure at 7 a.m. will almost always run higher than at 9 p.m. That is not a problem — it is normal physiology. Compare mornings to mornings, evenings to evenings.
Mistake 2: Measuring whenever you remember. Random timing injects too many variables — recent meals, movement, caffeine, stress — to produce reliable data.
Mistake 3: Reacting to a single reading. Clinical decisions are based on averages — typically 12 or more readings collected over three to seven days. A single spike at 150/95 does not diagnose hypertension. An average of 150/95 over two weeks is actionable data. [Shimbo et al., 2020]
Mistake 4: Measuring immediately after standing up. Even walking from the bedroom to the bathroom raises blood pressure transiently. Current AHA guidance specifies that at least five minutes of seated rest should elapse before the first reading, every time. [Pickering et al., 2005]
Mistake 5: Assuming a low evening reading means everything is fine. If morning averages are elevated but evening readings are normal, hypertension is still present — it is just masked at that time of day. Bring both data sets to your clinician.
Step-by-Step Blood Pressure Monitoring Protocol
Week 1 — Establishing Your Baseline
- Choose your two times: Morning within one hour of waking, before medications, coffee, or food. Evening one to two hours before bed, at least one hour after your last meal, alcohol, or exercise.
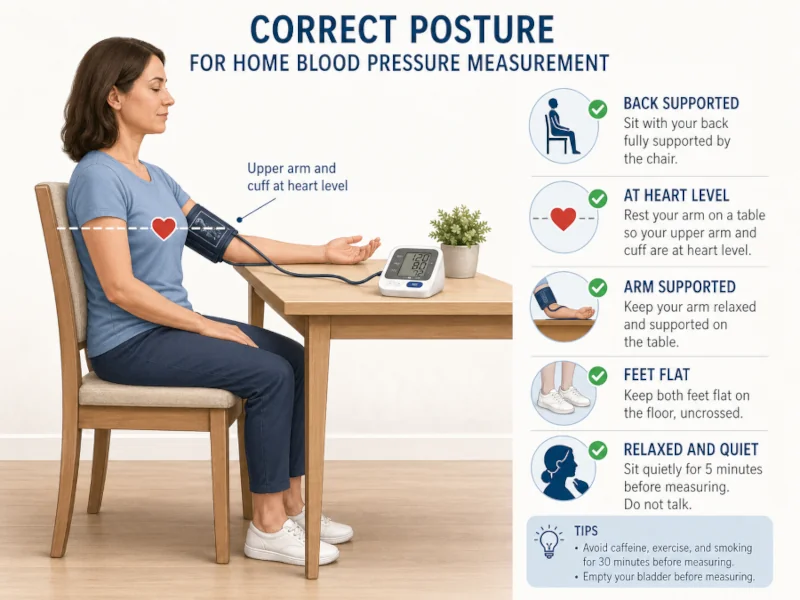
- Prepare identically each time: Empty bladder. Sit quietly for five minutes. Feet flat on floor. Back fully supported. Bare arm resting at heart level on a firm surface. No caffeine, nicotine, or exercise in the preceding 30 minutes. [Pickering et al., 2005]
- Take two readings, one to two minutes apart. Record both and average them. That average is your reading for that session.
- Do this twice daily for three to seven days. Three days (12 total readings) meets minimum clinical standards. Seven days is the gold standard for diagnosing hypertension via home monitoring. [Shimbo et al., 2020]
- Calculate separate averages: Average all morning readings. Average all evening readings. These two numbers matter far more than any individual measurement.
After Week 1 — Long-Term Maintenance
Once you have baseline data, most people with controlled blood pressure shift to one of these:
- Daily checks at one consistent time (usually morning) if blood pressure is stable and well-controlled
- Weekly paired checks (one morning, one evening) to confirm ongoing stability
- Full three-day protocols whenever medications change, readings shift unexpectedly, or your clinician requests a fresh assessment
Your clinician’s instructions take precedence. Ask them directly what schedule they need.
Special Situations
Before or after medication? Clinician preference varies. Some want pre-dose readings (to see whether the previous dose lasted); others want post-dose readings (to confirm the medication is working). Be consistent and document your choice so your clinician can interpret the data correctly.
What if you take blood pressure medication twice daily? Morning checks typically come before the morning dose. Evening checks can be taken before or after the evening dose — but stay consistent. Some prescribers want trough-level readings, taken just before the next scheduled dose, to confirm coverage lasts the full interval.
Before or after exercise? Always before. The AHA recommends avoiding exercise for at least 30 minutes before blood pressure measurement, as physical activity temporarily affects readings. [Pickering et al., 2005] Vigorous exercise may require a longer settling period of up to an hour. For context on how regular exercise influences blood pressure over time, see our exercise and blood pressure section.
Monitoring Schedules for Different Situations
| Protocol | When to use it | How it works |
| 3-Day Baseline (twice daily) | New diagnosis, starting home monitoring, recent medication change | Morning and evening for 3 consecutive days. Average each time separately. 12 total readings. |
| 7-Day Protocol (twice daily) | Suspected white-coat hypertension, borderline readings, validating home monitor | Morning and evening for 7 consecutive days. Discard Day 1. Average Days 2–7 (24 usable readings, 12 per time slot). |
| Once-Daily Maintenance | Controlled blood pressure, stable medications, routine tracking | One consistent time — usually morning. Check 3–4 days per week. Track weekly averages rather than individual readings. |

For Shift Workers and Non-Standard Schedules
Clock time matters less than physiological time. Cortisol peaks and blood pressure rhythms are anchored to the sleep-wake cycle, not the clock — so if your schedule rotates or you sleep during the day, base your measurements on your body’s rhythm, not the wall time. [Nakamura et al., 2021]
- Wake-time check: Within one hour of waking, regardless of whether that is 6 a.m. or 3 p.m. Before medications or caffeine. Sit quietly for five minutes first.
- Pre-sleep check: One to two hours before your normal sleep period, after your body has settled from the day’s activity and meals.
When recording readings, note the shift pattern — for example, “measured at wake +45 min on a night shift.” Your clinician can interpret variable-schedule data accurately with that context. For more on how sleep timing interacts with cardiovascular health, see our sleep and blood pressure guide.
How to Interpret Common Reading Patterns
| Pattern (over 3–7 days) | What it may indicate | Next step |
| Morning 10–20 mmHg higher than evening | Normal diurnal variation | Nothing. Expected physiology. |
| Morning 30+ mmHg higher than evening | Exaggerated morning surge; medication wearing off overnight | Discuss with clinician. May benefit from evening dosing or a longer-acting formulation. |
| Evening consistently higher than morning | Stress accumulation, high sodium intake, dehydration, or measurement error | Review daily habits and technique. Measure at true rest. |
| Both times consistently elevated | Uncontrolled or undertreated hypertension | Contact your clinician. Bring your full data log. |
| Both times consistently within target range | Blood pressure well controlled | Continue monitoring as directed. |
| Large day-to-day swings (20+ mmHg) | Inconsistent technique, disrupted sleep, high stress, or possible atrial fibrillation | Review technique first. If the pattern persists with correct technique, discuss with your clinician — automated oscillometric monitors are less reliable in atrial fibrillation and multiple readings or specialist assessment may be needed. |
These interpretations apply to patterns across three to seven days, not individual readings. Note on atrial fibrillation: automated oscillometric home BP monitors show increased reading-to-reading variability in people with AF; current guidance recommends taking at least three readings and flagging the pattern to your clinician. [Clark et al., 2019]
Consistent non-dipping — where BP fails to fall 10% overnight — has been associated with increased cardiovascular risk in multiple studies and is worth flagging if your clinician uses ambulatory monitoring to investigate your pattern. [Gavriilaki et al., 2020]
Pre-Measurement Checklist
Review this before every reading. These conditions are specified in AHA measurement guidelines. [Pickering et al., 2005]
- Bladder emptied
- Sitting quietly for 5 minutes — not just arrived from another room
- No caffeine, nicotine, or alcohol in the past 30 minutes
- No exercise in the past 30 minutes (vigorous exercise: allow at least 60 minutes)
- No food in the past 60 minutes (important for evening checks)
- Feet flat on floor, back fully supported — see proper BP monitoring technique for positioning details
- Arm bare (sleeve not bunched under cuff)
- Cuff at heart level — not resting on your lap
- Room temperature comfortable — cold rooms cause vasoconstriction and inflate readings
- Not talking or watching stimulating content during the measurement
- Same arm used every time (note which arm on your log)
- Two readings taken, one to two minutes apart — both recorded
- Same time of day, within a 30-minute window
What to Avoid Before and During Measurements
Do not check your blood pressure:
- Right after waking — sit still for 5 minutes first
- Within 30 minutes of caffeine or nicotine
- Within 30 minutes of exercise (60 minutes after vigorous activity)
- Within 60 minutes of a meal or alcohol
- While bursting to use the bathroom
- While talking, watching television, or feeling acutely stressed
- In a cold room
- With your arm unsupported or resting on your lap
Also avoid:
- Comparing readings from different times of day to gauge your trend
- Reacting to a single reading by adjusting medications or diet
- Retaking a reading immediately because you disliked the first number — anxiety will elevate the second one further
Why Weekly Averages Matter More Than Single Readings
Blood pressure fluctuates continuously. On a beat-to-beat basis, systolic pressure can vary markedly in response to breathing patterns, small movements, and passing thoughts — a well-documented physiological property of the cardiovascular system. [Schutte, Kollias & Stergiou, 2022]
A single high reading does not constitute hypertension. A single low reading does not mean treatment is working. Clinical guidelines define controlled blood pressure based on averages — typically 12 or more readings collected over three to seven days. That is why a consistent schedule and correct technique produce data that can actually guide clinical decisions. [Shimbo et al., 2020]
Practical example: You take seven morning readings over a week. Six fall between 125–135/80–85 mmHg. One reads 159/93. The outlier was probably caused by a full bladder, disrupted sleep, or hurrying through the prep steps. Average the other six. Your blood pressure is controlled. The 159 was noise, not signal — provided your technique was sound on the other six occasions.
FOR EDUCATIONAL PURPOSES ONLY: This article is not medical advice and does not replace guidance from a qualified healthcare professional. Blood pressure management is highly individual. People with diagnosed hypertension, heart disease, kidney disease, diabetes, pregnancy, or any condition affecting cardiovascular health should consult their clinician before making decisions based on home readings. Do not adjust or stop prescription medications based on home readings without speaking to your prescriber. If you experience a sudden severe headache, chest pain, shortness of breath, vision changes, or confusion alongside very high readings, seek emergency care immediately.
Frequently Asked Questions
Do I need to check both morning and evening readings forever?
No. After the initial baseline period — usually one to two weeks — most people with stable, controlled blood pressure switch to once-daily morning checks or weekly check-ins. Your clinician will specify what they need for ongoing management.
What if I forget a reading?
Skip it and resume your schedule the next day. Do not take extra readings to compensate — this disrupts the protocol and introduces inconsistency.
Can I check my blood pressure midday instead?
Yes, if you are consistent. Midday readings are valid when taken at the same time each day under the same resting conditions — not right after eating, moving, or experiencing stress. Morning and evening are preferred partly because they are easier to standardize around sleep and meals.
My evening reading is always lower than my morning reading. Does that mean my blood pressure is under control?
Not necessarily. If your morning average remains elevated while your evening readings look normal, you likely have hypertension that is simply less apparent in the evening. Bring both data sets to your clinician — evening readings alone can mask a problem.
Should I take my medication before or after my morning blood pressure check?
Ask your clinician. Pre-dose readings show whether the previous dose lasted through the night. Post-dose readings confirm the medication is working during its active phase. Document your choice consistently and tell your clinician which you chose.
I take my blood pressure pill at night. When should I check?
Morning readings show how well your overnight dose is covering the early-morning surge — the most pharmacologically demanding window. Evening readings taken before your nightly dose show your daytime coverage. Both are useful during the baseline period.
What if I work night shifts?
Anchor your checks to wake time and pre-sleep time rather than clock time. Cortisol and blood pressure rhythms follow your sleep-wake cycle regardless of when that cycle occurs. [Nakamura et al., 2021] Document your shift pattern alongside readings so your clinician can interpret the data correctly.
How long should I wait after waking before taking my blood pressure?
Within one hour of waking, but after five minutes of sitting quietly. If you wake at 6:30 a.m., you could measure any time between 6:35 a.m. and 7:25 a.m. Pick a specific window and keep it consistent.
References
- Kario K. Morning surge in blood pressure and cardiovascular risk: evidence and perspectives. Hypertension. 2010;56(5):765–773. doi:10.1161/HYPERTENSIONAHA.110.157149 → View source
- Shimbo D, Artinian NT, Basile JN, et al.; American Heart Association and American Medical Association. Self-measured blood pressure monitoring at home: a joint policy statement. Circulation. 2020;142(4):e42–e63. doi:10.1161/CIR.0000000000000803 → View source
- Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure measurement in humans: an AHA scientific statement. Circulation. 2005;111(5):697–716. doi:10.1161/01.CIR.0000154900.76284.F6 → View source
- Schutte AE, Kollias A, Stergiou GS. Blood pressure and its variability: classic and novel measurement techniques. Nat Rev Cardiol. 2022;19(10):643–654. doi:10.1038/s41569-022-00690-0 → View source
- Nakamura K, Miyoshi T, Yoshida M, et al. Cortisol on circadian rhythm and its effect on cardiovascular system. Int J Environ Res Public Health. 2021;18(2):676. doi:10.3390/ijerph18020676 → View source
- Clark CE, McDonagh STJ, McManus RJ; Blood Pressure Measurement Working Party of the British and Irish Hypertension Society. Measurement of blood pressure in people with atrial fibrillation. J Hum Hypertens. 2019;33(11):763–765. doi:10.1038/s41371-019-0261-4 → View source
- Gavriilaki M, Anyfanti P, Nikolaidou B, et al. Nighttime dipping status and risk of cardiovascular events in patients with untreated hypertension: a systematic review and meta-analysis. J Clin Hypertens. 2020;22(11):1951–1959. doi:10.1111/jch.14039 → View source