Herbs for the gallbladder and liver have been used for centuries to support bile flow and digestion, but only a handful are backed by serious clinical research. This guide ranks the best-studied options — milk thistle, artichoke leaf, turmeric, peppermint, and a few others — by the actual quality of human evidence, then explains how to use them safely, who should avoid them, and the symptoms that mean it’s time to put the herbs down and call a doctor.
Quick answer: which herbs actually have evidence
The short version, sorted by how strong the human research is:
- Best-studied for liver markers: milk thistle (silymarin) and artichoke leaf — both have multiple randomized trials, with mixed but generally favorable results for liver enzymes.
- Emerging clinical evidence: turmeric/curcumin for non-alcoholic fatty liver disease (NAFLD); peppermint oil for biliary-type indigestion.
- Strong traditional use, mostly preclinical evidence: dandelion root, rosemary, barberry, boldo.
- Use with extra caution: boldo (contains ascaridole, which is toxic in excess) and barberry (berberine has notable drug interactions).
None of these herbs cures liver disease or dissolves gallstones reliably. They support a working biliary system — they don’t replace medical care when something is actually wrong [NIDDK, 2025].
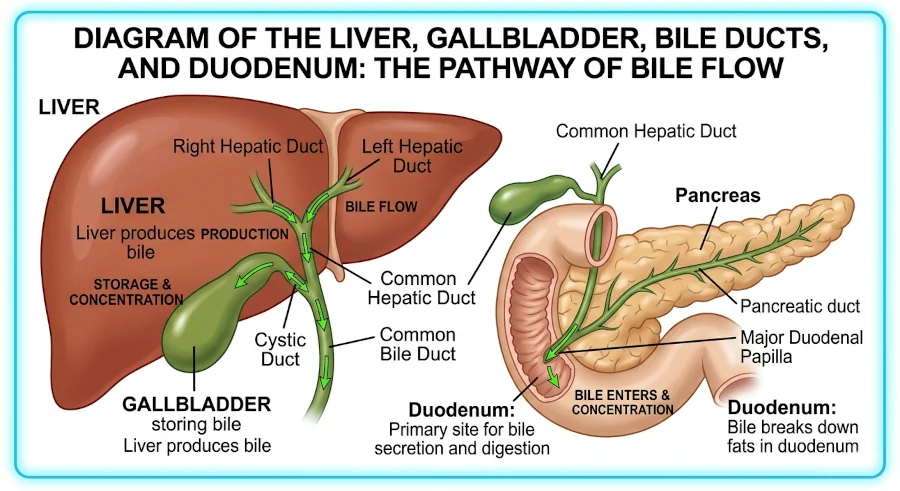
How the liver and gallbladder work together
The liver makes bile continuously. The gallbladder is a small storage pouch tucked under the liver that concentrates that bile and squirts it into the small intestine when a fatty meal arrives. Bile then emulsifies fat the way dish soap breaks up grease, so enzymes can digest it. Bile also carries cholesterol, bilirubin (a breakdown product of old red blood cells), and various waste compounds out of the body.
Two things go wrong most often. The liver gets overloaded — by alcohol, certain medications, viral hepatitis, or fat buildup in metabolic disease — and the gallbladder forms stones, usually when bile holds too much cholesterol or too little bile salt. Roughly 10–15% of adults in the United States have gallstones, though most never feel them [NIDDK, 2025].
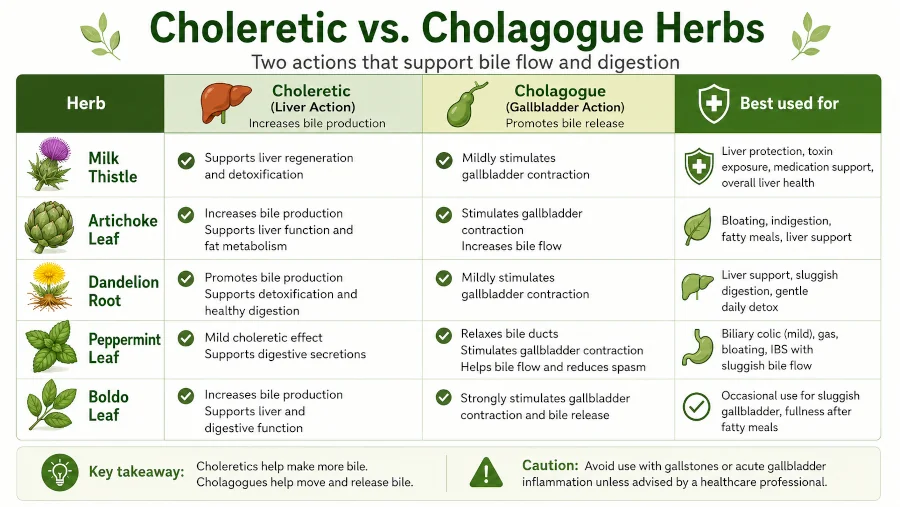
Choleretic vs cholagogue — what those terms mean
Two old herbal terms come up constantly in this topic:
- Choleretic plants increase the amount of bile the liver makes. Milk thistle, artichoke, dandelion, and turmeric sit here.
- Cholagogue plants stimulate the gallbladder to empty bile into the intestine, often by relaxing the sphincter of Oddi (the muscular valve at the bile duct’s exit). Peppermint, boldo, and rosemary act this way.
Many herbs do both. The practical takeaway: choleretics support sluggish bile production; cholagogues help when bile is being made but isn’t moving well, as in mild biliary-type dyspepsia (bloating and discomfort after fatty meals).
8 herbs for the gallbladder and liver, ranked by evidence quality
1. Milk thistle (Silybum marianum)
Milk thistle is the most-studied herb in this group. Its active extract, silymarin, is a mixture of flavonolignans — mainly silybin — that act as antioxidants and protect liver cells in lab and animal studies [NIH StatPearls, 2024]. In humans, results are more mixed: silymarin appears safe and is widely used by people with hepatitis C and NAFLD, but two NCCIH-funded trials did not show clear benefit for hepatitis C or non-alcoholic steatohepatitis [NCCIH, 2020]. Mayo Clinic’s summary calls the evidence for cirrhosis and hepatitis C “mixed” [Mayo Clinic, 2024].
Where it has a clearer role: intravenous silibinin is approved in Europe for poisoning from the death cap mushroom (Amanita phalloides), and oral silymarin is consistently well tolerated [LiverTox/NIH, 2020]. Typical oral doses in trials range from 250 to 750 mg of silymarin per day, divided in two or three doses.
Side effects are usually mild — bloating, gas, occasional loose stools. People allergic to ragweed, daisies, or marigolds should be cautious. For more on the plant itself, see our page on the milk thistle plant and silymarin.

2. Artichoke leaf (Cynara scolymus)
Globe artichoke leaf extract has been used for liver and gallbladder complaints since Roman times. The main compounds, cynarin and luteolin, increase bile output and may lower cholesterol. A randomized double-blind trial in 60 adults with non-alcoholic steatohepatitis (NASH) — fatty liver with inflammation — found that 2,700 mg of artichoke leaf extract daily for two months significantly reduced ALT, AST, total cholesterol, and triglycerides versus placebo [Rangboo et al., 2016]. That’s a small trial, but the effect size was meaningful and the design was clean.
Artichoke also has reasonable evidence in functional dyspepsia, especially the bloated, fat-intolerant kind people often describe as “my gallbladder doesn’t like me.” Standardized leaf extracts of 320–640 mg per day are typical. Bitter leaf preparations work better than eating the edible bracts, which contain less of the active compound. Our deeper write-up is on artichoke health benefits.
Avoid concentrated extracts if you have a known bile duct obstruction — pushing more bile through a blocked pipe is the wrong move.

3. Turmeric (Curcuma longa)
Turmeric’s active pigment, curcumin, is choleretic and anti-inflammatory. A 2023 umbrella meta-analysis pooling multiple reviews found that curcumin/turmeric supplementation in adults with NAFLD reduced ALT, AST, lipid markers, and BMI compared with placebo, with the strongest signals at curcumin doses near 1,000 mg per day [Ngu et al., 2023]. An earlier systematic review of four RCTs (228 participants) reached a similar conclusion: higher doses, longer duration, better liver-enzyme outcomes [Goodarzi et al., 2019].
Plain dietary turmeric is poorly absorbed. Most trials use a curcumin extract paired with piperine (from black pepper) or formulated as a phytosome to boost bioavailability. There’s one important caveat: rare cases of curcumin-related liver injury have been reported, especially with high-dose supplements in people with underlying liver issues. Treat curcumin as a supplement with a real effect — useful in mild NAFLD, but worth running past a doctor if you already take liver-relevant medications.
More on culinary and medicinal uses on our turmeric plant health benefits page.
4. Peppermint (Mentha × piperita)
Peppermint earns its place mostly as a cholagogue and antispasmodic. Menthol relaxes smooth muscle, including the sphincter of Oddi, which can help when bile flow is sluggish and meals feel heavy. A 2018 review concluded that peppermint oil is supported by placebo-controlled trials in irritable bowel syndrome, functional dyspepsia, and post-operative nausea, with a good safety profile [Chumpitazi et al., 2018]. Animal work also shows peppermint oil increases bile and bile-acid output in the rat liver model [Zong et al., 2011].
Enteric-coated capsules of 0.2–0.4 mL peppermint oil twice daily are the usual research dose. A simple after-meal cup of peppermint tea is gentler and may be enough for mild bloating. Peppermint can worsen reflux, so people with significant GERD should be cautious.
Full plant profile on our peppermint plant benefits page.
5. Dandelion (Taraxacum officinale)
Dandelion root is a classic bitter, traditionally used as a “liver tonic” in European, Chinese, and Indian medicine. Multiple lab and animal studies show it protects liver tissue against alcohol-, paracetamol-, and carbon-tetrachloride-induced damage, and it acts as both choleretic and cholagogue [Olas, 2025]. The catch is that well-controlled human trials are scarce, so the evidence sits one rung below milk thistle and artichoke.
For everyday support, dandelion root tea or a 500–1,500 mg/day extract is the usual range. Roasted dandelion root makes a passable coffee substitute. People allergic to ragweed family plants should approach with care. See our overview of the dandelion plant for traditional preparations.
6. Rosemary (Salvia rosmarinus)
Rosemary has long appeared in European cholagogue formulas. Its key compounds — rosmarinic acid, carnosol, and carnosic acid — have antioxidant activity and increase bile flow in animal models. Human clinical evidence specific to the liver and gallbladder is limited, so its role is supportive rather than starring. As a culinary herb it’s a low-risk, high-flavor way to season fatty meals; as a tea, 1–2 teaspoons of dried leaf in hot water after a heavy dinner is a traditional choice. More on our benefits of rosemary page.
7. Boldo (Peumus boldus)
Boldo is approved as a traditional herbal medicine in Europe for mild digestive complaints. It’s a strong cholagogue, mostly thanks to the alkaloid boldine. But boldo leaf also contains ascaridole, a volatile compound that is toxic to the liver in excess. The clinical guidance is unambiguous: short courses only (typically no more than 2–4 weeks), ascaridole-free preparations if you can find them, and complete avoidance in pregnancy, breastfeeding, gallstone disease with obstruction, or existing liver disease [Drugs.com, 2024].
Boldo is useful — but it’s the herb on this list with the narrowest safety margin. If you’re new to it, talk with a clinician before starting. Background on the plant: boldo health benefits.
8. Barberry (Berberis vulgaris)
Barberry root bark contains berberine, the same alkaloid found in goldenseal and Oregon grape. Berberine has genuine biological activity — it improves blood sugar and lipid markers and may reduce bile cholesterol saturation — but it also inhibits CYP3A4, the same liver enzyme that handles statins, immunosuppressants, certain anticoagulants, and many other prescriptions. The result: barberry has real benefits and real interaction risks. People on multiple medications should not self-prescribe it.
Quick reference: choleretic vs cholagogue at a glance
How the herbs in this article cluster by action and how strong the human evidence is right now.
| Herb | Choleretic | Cholagogue | Best use | Human evidence |
| Milk thistle | ✓ | — | Liver-cell support, toxin exposure | Strongest body of trials; results for chronic liver disease are mixed |
| Artichoke leaf | ✓ | ✓ | Fatty liver, fat-related indigestion, high cholesterol | Multiple RCTs; one positive NASH trial |
| Turmeric / curcumin | ✓ | — | NAFLD, low-grade liver inflammation | Growing — meta-analyses favor curcumin at higher doses |
| Peppermint | Mild | ✓ | Biliary-type dyspepsia, post-meal heaviness | Good for dyspepsia/IBS; biliary-specific evidence is mostly preclinical |
| Dandelion | ✓ | ✓ | Everyday digestive support, bitters | Mostly animal and lab data |
| Rosemary | Mild | ✓ | Culinary support for fatty meals | Limited |
| Boldo | ✓ | ✓ | Short-term dyspepsia (clinician-guided) | Traditional approval; safety concerns |
| Barberry | ✓ | — | Bile composition (limited niche) | Berberine has trials; drug-interaction risk |
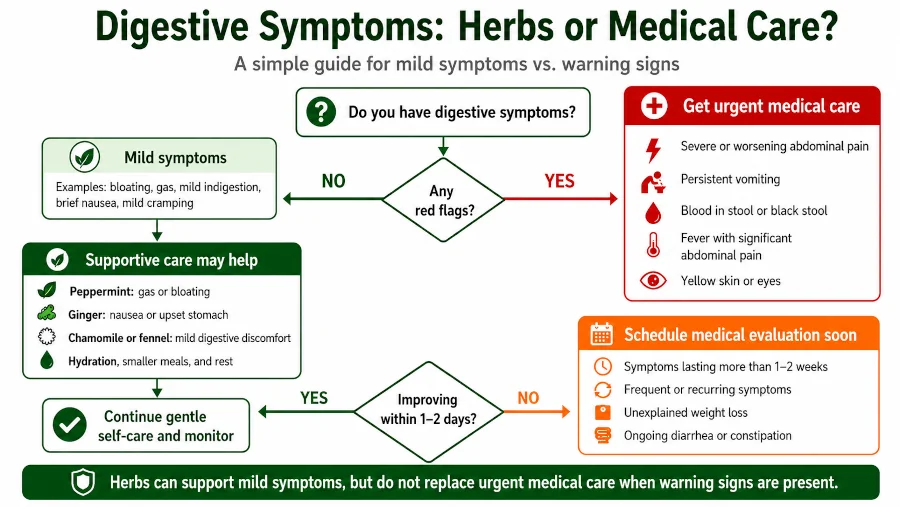
Red-flag symptoms: when to skip herbs and call a doctor
These symptoms mean go to urgent care or the ER — not the herb cabinet [Mayo Clinic, 2024]:
- Severe pain in the upper right abdomen, especially pain that wakes you up or you can’t sit still through
- Pain radiating to the right shoulder or between the shoulder blades that lasts more than a couple of hours
- Yellowing of the skin or whites of the eyes (jaundice)
- Fever or chills with abdominal pain — possible bile duct infection
- Pale or clay-colored stools combined with dark urine
- Persistent nausea and vomiting that prevents keeping fluids down
Gallstones are common but obstruction can become a surgical emergency quickly. Hepatitis, bile duct stones, and cholangitis can mimic ordinary indigestion in the first hours.
Safety, side effects, and drug interactions
Most of the herbs here are well tolerated in normal culinary or tea doses. Concentrated extracts are where caution earns its keep.
Common side effects to know
- Milk thistle: mild GI symptoms (gas, bloating, loose stools); allergic reactions in people sensitive to ragweed-family plants
- Artichoke leaf: gas, gut grumbling, rare allergic reactions
- Turmeric/curcumin: occasional stomach upset; rarely, reports of idiosyncratic liver injury at high doses
- Peppermint oil: heartburn or reflux, especially without enteric coating; anal burning in IBS preparations
- Boldo: avoid prolonged use; ascaridole can be hepatotoxic in excess
- Barberry / berberine: GI upset; significant CYP3A4 drug-interaction potential
Medication interactions worth flagging
Talk to a pharmacist before combining these herbs with prescription drugs. Particularly relevant interactions include:
- Anticoagulants (warfarin, apixaban) — turmeric, milk thistle, and several others can theoretically increase bleeding risk
- Diabetes medications — milk thistle and berberine can lower blood sugar; doses may need adjustment
- Statins, immunosuppressants, certain antifungals, some antidepressants — berberine (barberry) and concentrated curcumin can alter metabolism via CYP enzymes
- Estrogens and tamoxifen — milk thistle should be discussed in hormone-sensitive cancers
Who should avoid these herbs
- Pregnant or breastfeeding people. Boldo, barberry, and high-dose curcumin are typically avoided. Milk thistle and artichoke lack robust safety data in pregnancy and should only be used with a clinician’s guidance.
- Anyone with bile duct obstruction or active biliary colic. Cholagogues push bile through a system that’s already blocked — that’s the wrong direction.
- People with acute or advanced liver disease. Any herb taken in concentrated form is metabolized by an already-stressed liver. Run it past a hepatologist.
- Children under 18. Most dosing research is in adults. Use only under pediatric guidance.
- Anyone on multiple prescription medications. The more drugs you take, the higher the odds of an interaction.
Realistic expectations
Herbs for the gallbladder and liver are best understood as digestive support, not cures. Here’s what the evidence reasonably supports — and what it does not.
- Reasonable: milder post-meal bloating, smoother fat digestion, modest improvements in liver enzymes in NAFLD over weeks to months, easier transit during dyspeptic episodes.
- Unrealistic: dissolving existing gallstones, reversing cirrhosis, “detoxing” a healthy liver, replacing antiviral or surgical treatment for confirmed disease.
Lifestyle changes do more heavy lifting than any herb: keeping a stable weight (rapid weight loss is itself a gallstone risk factor), eating enough fiber, going easy on alcohol, and managing diabetes and lipid problems matter more than any tea or capsule [Johns Hopkins Medicine, 2024]. For a hands-on look at lifestyle approaches, see our piece on natural remedies for gallstones, and for the wider digestive picture, herbs for the digestive system.
| Health Disclaimer This article is for educational and informational purposes only. It is not medical advice and is not a substitute for diagnosis or treatment by a qualified clinician. Herbs can interact with prescription and over-the-counter medicines, and some are unsafe in pregnancy, breastfeeding, or with certain health conditions. Do not stop or change any prescribed treatment based on this article. If you have liver or gallbladder symptoms — pain in the upper right abdomen, jaundice (yellow skin or eyes), fever with chills, vomiting, or pale stools with dark urine — speak with a doctor before using herbal remedies, and seek urgent care if symptoms are severe or worsening. |
Frequently Asked Questions
Are herbs for the gallbladder and liver safe if I already have gallstones?
Sometimes. Mild cholagogue herbs at culinary doses (a cup of peppermint or dandelion tea) are usually fine. Concentrated cholagogue extracts — especially boldo — can theoretically push a stone toward the bile duct, where it can lodge. If you have known gallstones, talk to a doctor before starting any extract.
Can milk thistle reverse fatty liver?
Milk thistle may modestly lower elevated liver enzymes in NAFLD in some trials, but it does not reverse fatty liver on its own. The lifestyle pieces — weight loss, exercise, reducing alcohol — drive most of the change. Treat milk thistle as a supportive add-on, not a treatment.
How long does it take to see results?
If something is going to work for digestive symptoms (bloating, fat intolerance), most people notice a change within one to four weeks. For liver-enzyme improvements, trials typically run two to six months. If nothing has changed after eight weeks of consistent use, the herb probably isn’t doing what you hoped.
Is a “liver cleanse” or “liver flush” the same thing?
No, and there’s no evidence the common olive oil and lemon juice “flush” actually expels gallstones. The greenish blobs that appear afterward are saponified oil, not stones. The herbs in this article support normal bile function — they don’t “flush” anything.
Can I take more than one of these herbs together?
Combination formulas (milk thistle + artichoke + dandelion, for example) are common and generally well tolerated, but stacking concentrated extracts increases the chance of interactions and side effects. A good rule: start one herb at a time, give it at least two weeks, and add others only with reason.
Related reading on this site
- The milk thistle plant and silymarin
- Artichoke health benefits
- Turmeric plant health benefits
- The dandelion plant
- Peppermint plant benefits
- Boldo health benefits
- Benefits of rosemary
- Natural remedies for gallstones
- Herbs for the digestive system
References
- Mount Sinai Health System. Division of Liver Diseases — services and conditions. 2025. → View source
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Gallstones — Definition & Facts. 2025. → View source
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Gallstones — overview. 2025. → View source
- Mayo Clinic. Gallstones: symptoms and causes. 2025. → View source
- National Center for Complementary and Integrative Health (NCCIH). Milk thistle: usefulness and safety. 2020. → View source
- Mayo Clinic. Milk thistle (silymarin) — drugs and supplements. 2024. → View source
- LiverTox / National Institutes of Health. Milk thistle (Silymarin). 2020. → View source
- Bijak M, et al. Milk Thistle — StatPearls. NCBI Bookshelf, 2024. → View source
- Rangboo V, et al. The effect of artichoke leaf extract on alanine aminotransferase and aspartate aminotransferase in patients with nonalcoholic steatohepatitis. International Journal of Hepatology, 2016 (PMC4879230). → View source
- Olas B. The role of dandelion (Taraxacum officinale) in liver health and hepatoprotective properties — narrative review. PubMed, 2025. → View source
- Ngu MH, et al. Effects of curcumin/turmeric supplementation on liver enzymes, lipid profiles, glycemic index, and anthropometric indices in NAFLD: an umbrella meta-analysis. PubMed, 2023. → View source
- Goodarzi R, et al. Efficacy of curcumin/turmeric on liver enzymes in patients with non-alcoholic fatty liver disease: a systematic review of RCTs. PubMed, 2019. → View source
- Chumpitazi BP, Kearns GL, Shulman RJ. Review article: the physiological effects and safety of peppermint oil and its efficacy in irritable bowel syndrome and other functional disorders. PubMed, 2018. → View source
- Zong L, et al. Preliminary experimental research on the mechanism of liver bile secretion stimulated by peppermint oil. Journal of Digestive Diseases, 2011. → View source
- Drugs.com. Boldo (Peumus boldus) — uses, benefits, and dosage. 2024. → View source
- Johns Hopkins Medicine. Gallstones — risk factors and overview. 2025. → View source
- UCSF Department of Surgery. Gallstones. 2024. → View source