If you’ve just been told you have a hiatal hernia, you probably have two worries running at once: Is this serious? and Will I need surgery? The short answer, for most people, is reassuring. Most hiatal hernias are small, cause few or no symptoms, and can be managed without an operation. But some do need repair, and knowing the difference matters.
This guide walks through the full range of hiatal hernia treatment options, explains when surgery is usually considered, addresses the common question of what size hiatal hernia needs surgery, and covers a detail many people search for after an operation is scheduled: hiatal hernia surgery and chocolate. The goal is to reduce the confusion and give you something useful to bring into your next conversation with your doctor.
What a Hiatal Hernia Actually Is
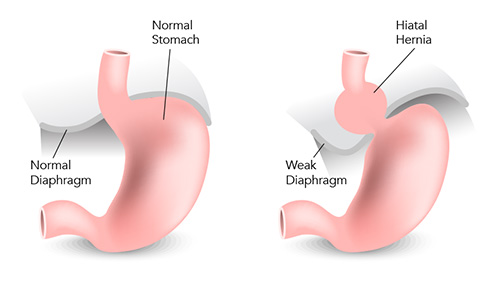
A hiatal hernia happens when part of the stomach pushes up through a small opening in the diaphragm called the hiatus, where the esophagus normally passes through on its way to the stomach [Cleveland Clinic, 2023]. The diaphragm is the flat muscle that separates your chest from your abdomen, and the hiatus is its weak point.
Hiatal hernias are common, especially with age, and many are discovered by accident during imaging for something else [Mayo Clinic, 2025].
The four types
Doctors classify hiatal hernias into four types based on anatomy [SAGES, 2013]:
- Type I — Sliding hernia. The gastroesophageal junction slips above the diaphragm. This is the most common form, accounting for about 95% of cases.
- Type II — Pure paraesophageal. The junction stays in place, but part of the stomach squeezes up alongside the esophagus.
- Type III — Mixed. A combination of Types I and II. Most paraesophageal hernias are actually Type III.
- Type IV — Complex. A larger defect lets other organs (such as colon, small bowel, or spleen) slip into the chest cavity alongside the stomach.
The type matters because sliding hernias usually cause reflux symptoms, while paraesophageal hernias carry a higher risk of mechanical complications such as obstruction or, rarely, twisting of the stomach [Yeh & Korn, 2021].
Hiatal Hernia Treatment Options at a Glance
Treatment is almost always tailored to symptoms and hernia type rather than to the image on a scan alone. There is a ladder of options, and most people never need to climb past the first two rungs.
Lifestyle changes
For a sliding hiatal hernia with mild reflux, lifestyle adjustments often do most of the work:
- Eating smaller, more frequent meals
- Avoiding eating within about three hours of bedtime
- Elevating the head of the bed by 6–8 inches
- Losing excess weight if applicable
- Limiting known reflux triggers (more on those later)
- Quitting smoking and moderating alcohol [Mayo Clinic, 2025; NIDDK, 2020]
These steps sound basic, but in clinical practice they are often underused, and they can meaningfully reduce heartburn and regurgitation.

Medications
If lifestyle changes aren’t enough, the next step is usually medication to reduce stomach acid or protect the esophagus:
- Antacids for occasional, mild symptoms
- H2 receptor blockers (such as famotidine) for moderate symptoms
- Proton pump inhibitors (PPIs) for more persistent reflux [ACG, Katz et al., 2022]
Medication doesn’t fix the hernia itself. It addresses the reflux the hernia is causing. For many people with Type I hernias, that’s all they’ll ever need.
Endoscopic and minimally invasive procedures
For select patients with GERD who don’t want long-term medication but aren’t ready for traditional surgery, newer options exist, such as magnetic sphincter augmentation (the LINX device) and transoral incisionless fundoplication. These are usually considered in cases where the hernia is small and reflux is the main problem [ACG, Katz et al., 2022].
Surgical repair
When a hernia is large, symptomatic, or causing complications, surgery becomes the main option. The standard repair involves:
- Pulling the stomach back down into the abdomen
- Tightening the hiatus, sometimes with mesh reinforcement
- Performing a fundoplication — wrapping the top of the stomach around the lower esophagus to strengthen the barrier against reflux [SAGES, Daly et al., 2024]
Most repairs today are done laparoscopically or robotically, using several small incisions. Recovery is generally faster than open surgery, with shorter hospital stays and less pain [SAGES, 2013].
When Does a Hiatal Hernia Need Surgery?
This is the heart of the question for most people, and the honest answer is: it depends on what the hernia is doing, not just what it looks like.
Symptoms and complications that push toward surgery
Surgery is typically considered when one or more of these are present [SAGES, Daly et al., 2024; Mayo Clinic, 2019]:
- Reflux that doesn’t respond adequately to medication and lifestyle changes
- Severe esophagitis (inflammation of the esophagus) despite treatment
- Difficulty swallowing caused by the hernia
- Chest pain or pressure after meals from a large paraesophageal hernia
- Iron-deficiency anemia linked to a giant paraesophageal hernia (from slow bleeding at sites of mucosal irritation) [Carrott et al., 2013]
- Recurrent aspiration or breathing problems thought to be reflux-related
- Barrett’s esophagus or other evidence of ongoing injury
For paraesophageal hernias (Types II–IV) that are causing symptoms, repair is generally recommended because the risk of future complications is meaningful [SAGES, 2013].
Emergency situations

Rarely, a paraesophageal hernia can twist on itself — a condition called gastric volvulus — or get trapped, cutting off blood supply. Warning signs include sudden severe chest or upper abdominal pain, inability to vomit, and difficulty swallowing even liquids. This is a medical emergency and needs immediate care [SAGES, 2013].
It’s worth noting the modern shift in thinking: in the past, doctors often recommended repairing every paraesophageal hernia, even without symptoms. Newer evidence suggests that watchful waiting is reasonable in many asymptomatic or minimally symptomatic patients, especially those who are older or have other medical conditions, because the risk of an emergency turns out to be lower than once thought [Stylopoulos et al., 2002; SAGES, Daly et al., 2024].
What Size Hiatal Hernia Needs Surgery?
There is no universal size cutoff. A hernia isn’t like a blood pressure reading that flips from “fine” to “operate” at a specific number.
That said, size does factor in. Hernias roughly 5 cm or larger are often described as “large,” and these are more likely to be paraesophageal, more likely to cause mechanical symptoms, and more likely to be repaired when they are causing problems [Kohn et al., 2013]. Very large, or “giant,” paraesophageal hernias — typically those where more than about a third of the stomach sits in the chest — are the ones most often linked to complications like chronic bleeding or volvulus.
Why size is part of the picture, not the whole picture
The decision to repair usually depends on a combination of factors:
- Symptoms — how much is the hernia actually affecting daily life?
- Type — sliding versus paraesophageal
- Complications — esophagitis, anemia, aspiration, obstruction
- Anatomy — how much of the stomach has migrated, the shape of the defect
- Overall health — age, other conditions, surgical risk
- Patient preferences — especially for borderline cases
A small hernia causing severe reflux may need repair. A moderately large one causing no problems in an older adult may be safely monitored. The SAGES 2024 guidelines specifically highlight shared decision-making between the patient and the surgical team as the right way to navigate gray areas [SAGES, Daly et al., 2024].
Comparison Table: Treatment Path by Situation
| Situation | Typical First-Line Approach | When Surgery Is Considered |
| Small sliding hernia, no symptoms | No treatment needed | Rarely |
| Sliding hernia with mild heartburn | Lifestyle changes, antacids | If symptoms persist despite treatment |
| Sliding hernia with moderate/severe GERD | PPIs, lifestyle changes | If medication fails or complications develop |
| Asymptomatic paraesophageal hernia | Watchful waiting in many cases | Shared decision, especially if symptoms develop |
| Symptomatic paraesophageal hernia | Evaluation for repair | Usually recommended |
| Large/giant paraesophageal hernia with complications | Referral to surgical team | Generally recommended |
| Acute obstruction or gastric volvulus | Emergency care | Emergency surgery |
This table is a general guide, not a medical recommendation for your individual case.
Can Chiropractic Care Help a Hiatal Hernia?
This is one of the most common questions people ask after a hiatal hernia diagnosis, usually because they’ve read about a manual technique sometimes called a “stomach pull-down” or “hiatal hernia maneuver.” It’s a fair question, and it deserves a careful answer.
Chiropractic care is not a standard or proven treatment for hiatal hernia. Major medical organizations, including the Society of American Gastrointestinal and Endoscopic Surgeons and the American College of Gastroenterology, do not list chiropractic manipulation as a recognized treatment in their clinical guidelines [SAGES, Daly et al., 2024; ACG, Katz et al., 2022]. The available published research on manual techniques for hiatal hernia is limited to case reports and small observational write-ups rather than rigorous clinical trials, which means the evidence base is weak and the effect — if any — is hard to measure.
That said, some people do report short-term symptom relief after manual abdominal techniques, diaphragmatic release work, or stress- and posture-related care. It’s biologically plausible that relaxing the diaphragm and surrounding muscles could ease discomfort for some patients. What’s not established is whether any of this actually repositions the stomach in a lasting way or changes the underlying anatomy of the hernia. In most cases, it’s more accurate to think of any benefit as symptomatic rather than corrective.
For most readers, the practical takeaway is this: hiatal hernia treatment decisions are driven by the type of hernia, the severity of symptoms, the presence of reflux or complications, and your overall health — not by manual manipulation. Lifestyle changes, medications, and, when needed, surgical repair remain the mainstays of care.
It’s also important to know when chiropractic care is clearly not the right path. Seek medical evaluation promptly if you have any of the following:
- Chest pain or pressure, especially if sudden or severe
- Difficulty swallowing, or food feeling “stuck”
- Persistent vomiting or inability to keep liquids down
- Vomiting blood or passing black, tarry stools
- Unintentional weight loss or new anemia
- Severe or worsening reflux despite treatment
- A known large or paraesophageal hernia with new symptoms
If you’re considering any complementary approach for mild symptoms, the safest path is to do it alongside appropriate medical evaluation — not instead of it — and to make sure your diagnosis is confirmed first.
Key points – Chiropractic care is not a proven or standard treatment for hiatal hernia, and major medical guidelines don’t include it. – Some people report short-term symptom relief from manual techniques, but the evidence is limited to case reports, not rigorous trials. – Treatment decisions should be based on hernia type, symptoms, and complications — usually lifestyle changes, medication, or surgery. – Red-flag symptoms (severe chest pain, trouble swallowing, vomiting, GI bleeding) need prompt medical evaluation, not alternative care.
Recovery After Hiatal Hernia Surgery
Most people go home within 1–2 days after laparoscopic repair and return to light activities in about two weeks, with full recovery typically in 4–6 weeks [Cleveland Clinic, 2023]. The biggest rules during recovery are to protect the fresh repair and to avoid anything that could trigger forceful retching or vomiting, which can physically disrupt the stitches before scar tissue has formed [DeMeester, via Pacific Hernia Center, 2024].
The post-op diet stages
Most surgical teams use a staged diet, though exact timelines vary:
- Clear liquids for the first day or two
- Full liquids (broth, smooth soups, protein shakes) for roughly 1–2 weeks
- Soft, moist foods (eggs, yogurt, mashed vegetables, well-cooked fish) for another few weeks
- Gradual return to solids, avoiding dry, crumbly, sticky, or fibrous textures at first
The fundoplication wrap is typically swollen for several weeks, which narrows the lower esophagus temporarily and makes it easy for solid food to get stuck. That’s why the diet is advanced slowly.
Hiatal Hernia Surgery and Chocolate: Why It’s Usually Off the Menu
Chocolate comes up often in post-op instructions, and for good reasons that go beyond cravings.
- It relaxes the lower esophageal sphincter. Chocolate contains methylxanthines (compounds related to caffeine), and classic studies going back decades have shown that chocolate lowers the pressure of the lower esophageal sphincter, the muscular barrier that keeps stomach contents from refluxing [Wright & Castell, 1975; Nebel & Castell, 1973]. A freshly repaired hiatus and a new fundoplication are working hard to recreate that barrier; anything that loosens it runs counter to the point of the surgery.
- It’s high in fat. Fat slows stomach emptying and can worsen reflux. It can also contribute to nausea in the early post-op period [Healthline, 2024].
- It can be surprisingly hard to swallow. Solid chocolate can be sticky and can soften into a thick paste that doesn’t move easily through a swollen fundoplication.
- Caffeine stimulates acid production. Even small amounts in dark chocolate can add to symptoms.
Can you eat chocolate after hiatal hernia surgery?
Not in the early recovery period. For the first several weeks, most surgeons recommend avoiding chocolate entirely, along with other common reflux triggers. As healing progresses and your surgeon clears you to return to a regular diet, many people can reintroduce small amounts of chocolate and see how they tolerate it. Some go back to enjoying it without trouble; others find that even a square of dark chocolate brings symptoms back.
There is meaningful individual variation here. Your surgeon’s specific instructions matter more than any general rule, and the honest answer to “can I have chocolate?” is usually “eventually, in moderation, if it doesn’t cause symptoms.”
Other Foods to Approach Carefully After Surgery
Along with chocolate, common items to limit during the recovery window include:
- Carbonated drinks (gas can be trapped behind the wrap and cause painful bloating)
- Coffee and strong tea
- Alcohol
- Citrus and tomato-based foods
- Spicy dishes
- Fried and very fatty foods
- Peppermint
- Tough meats, raw vegetables, bread with dense crust, and other foods that don’t swallow easily in the early weeks [NIDDK, 2020; Cleveland Clinic, 2023]
Most people find they can reintroduce many of these over time. Keeping a simple food and symptom log during recovery is one of the most useful things you can do.
When to Call a Doctor

Call your care team or seek urgent evaluation if you experience:
- Severe chest or upper abdominal pain, especially if it comes on suddenly
- Inability to swallow even liquids
- Persistent vomiting or retching
- Vomiting blood or passing black, tarry stools
- High fever after surgery
- Shortness of breath or new heart-related symptoms
- Signs of infection at an incision site (redness, warmth, pus, spreading tenderness)
- Reflux symptoms that worsen sharply or return suddenly after feeling well
Sudden severe pain after a known paraesophageal hernia, particularly with difficulty vomiting, should be treated as a potential emergency [SAGES, 2013].
Practical Next Steps
If you are still figuring out where you stand, a reasonable approach is:
- Write down your symptoms — what, when, how often, and how severe.
- Note anything that makes them better or worse, including foods.
- Ask your clinician what type of hiatal hernia you have and whether tests like an upper endoscopy, barium swallow, or pH/manometry study would help clarify things.
- Ask specifically whether lifestyle changes and medication are worth a structured trial before considering surgery.
- If surgery is on the table, ask about the surgeon’s volume, expected recovery, and what the post-op diet will look like for you.
Most people leave that conversation with a clearer plan than they went in with.
Medical disclaimer: This article is for general information and education. It is not medical advice and not a substitute for individualized evaluation, diagnosis, or treatment by a qualified healthcare professional. If you have symptoms or a diagnosed hiatal hernia, talk with your doctor about the right next steps for your specific situation.
Frequently Asked Questions
Is a hiatal hernia dangerous?
Most are not. Small sliding hernias are very common and often cause no problems. Larger paraesophageal hernias carry a higher risk of complications and are the ones doctors watch more closely [Cleveland Clinic, 2023].
Can a hiatal hernia heal on its own?
No. A hiatal hernia is an anatomical change, not an inflammation, so it doesn’t heal. But the symptoms it causes can often be controlled well with lifestyle changes and medication, which is why many hernias never need any intervention at all [Mayo Clinic, 2025].
What size hiatal hernia needs surgery?
There isn’t a fixed size cutoff. Hernias around 5 cm or larger are more often called “large,” and very large paraesophageal hernias are more likely to need repair, but the decision is based on symptoms, type, complications, and your overall health — not size alone [Kohn et al., 2013; SAGES, Daly et al., 2024].
Can you eat chocolate after hiatal hernia surgery?
Not during early recovery. Chocolate relaxes the lower esophageal sphincter, is high in fat, and can be hard to swallow over a swollen fundoplication. Most surgeons recommend avoiding it for several weeks. Later, many patients can reintroduce small amounts if they tolerate it [Wright & Castell, 1975; Pacific Hernia Center, 2024].
How long does hiatal hernia surgery recovery take?
Most people return to light activities within about two weeks and to full activity around 4–6 weeks, though the diet is usually advanced slowly over roughly 6 weeks [Cleveland Clinic, 2023].
Will surgery cure my reflux?
Often, yes — especially when done for the right reasons. A well-performed repair with fundoplication significantly reduces reflux for most patients, though some people still need occasional medication afterward, and a small number have persistent symptoms [SAGES, Daly et al., 2024].
References
- Cleveland Clinic. Hiatal Hernia: What It Is, Symptoms, Treatment & Surgery. Reviewed 2023. https://my.clevelandclinic.org/health/diseases/8098-hiatal-hernia
- Mayo Clinic. Hiatal hernia — Diagnosis and treatment. Updated 2025. https://www.mayoclinic.org/diseases-conditions/hiatal-hernia/diagnosis-treatment/drc-20373385
- Mayo Clinic News Network. Mayo Clinic Q and A: Surgery for hiatal hernias. 2019. https://newsnetwork.mayoclinic.org/discussion/mayo-clinic-q-and-a-surgery-for-hiatal-hernias/
- SAGES (Daly S, Kumar SS, Collings AT, et al.). Guidelines for the Surgical Treatment of Hiatal Hernias. Surgical Endoscopy, 2024. https://www.sages.org/publications/guidelines/guidelines-for-the-surgical-treatment-of-hiatal-hernias/
- SAGES (Kohn GP, Price RR, DeMeester SR, et al.). Guidelines for the management of hiatal hernia. Surgical Endoscopy, 2013;27:4409–4428.
- Katz PO, Dunbar KB, Schnoll-Sussman FH, et al. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. American Journal of Gastroenterology, 2022;117:27–56.
- Stylopoulos N, Gazelle GS, Rattner DW. Paraesophageal hernias: operation or observation? Annals of Surgery, 2002;236:492–501.
- Carrott PW, Markar SR, Hong J, et al. Iron-deficiency anemia is a common presenting issue with giant paraesophageal hernia and resolves following repair. Journal of Gastrointestinal Surgery, 2013;17:858–862.
- Wright LE, Castell DO. The adverse effect of chocolate on lower esophageal sphincter pressure. Digestive Diseases and Sciences, 1975. https://link.springer.com/article/10.1007/BF01070826
- Nebel OT, Castell DO. Inhibition of the lower esophageal sphincter by fat — a mechanism for fatty food intolerance. 1973.
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Acid Reflux (GER & GERD) in Adults — Eating, Diet, & Nutrition. https://www.niddk.nih.gov/health-information/digestive-diseases/acid-reflux-ger-gerd-adults/eating-diet-nutrition
- Pacific Hernia Center (DeMeester S). Why No Chocolate After Hiatal Hernia Surgery. 2024. https://pacifichernia.com/why-no-chocolate-after-hiatal-hernia-surgery/
- Healthline. Can You Eat Chocolate If You Have Acid Reflux? Reviewed 2024. https://www.healthline.com/health/digestive-health/chocolate-and-acid-reflux