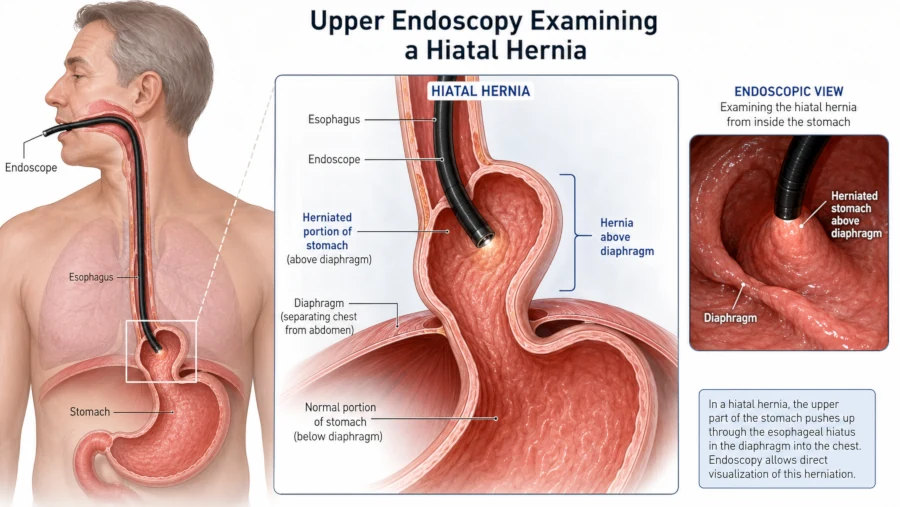
Hiatal hernia endoscopy — more formally called an upper endoscopy or esophagogastroduodenoscopy (EGD) — is the most direct way for a doctor to look inside the esophagus and stomach and confirm whether a hiatal hernia is present, how large it is, and whether it has caused any damage to the surrounding tissue. If you have been experiencing persistent heartburn, acid reflux, difficulty swallowing, or chest discomfort, and your doctor suspects a hiatal hernia, an EGD is likely to be part of the workup.
This article explains what happens during a hiatal hernia endoscopy, how reliable it is, how to prepare, what the risks are, and what comes next after you receive results. It is written for people who want clear, medically accurate information before their procedure.
What Is a Hiatal Hernia?
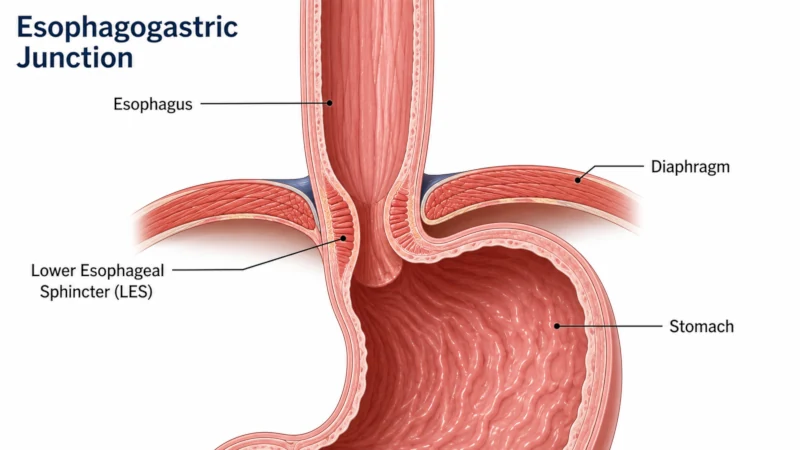
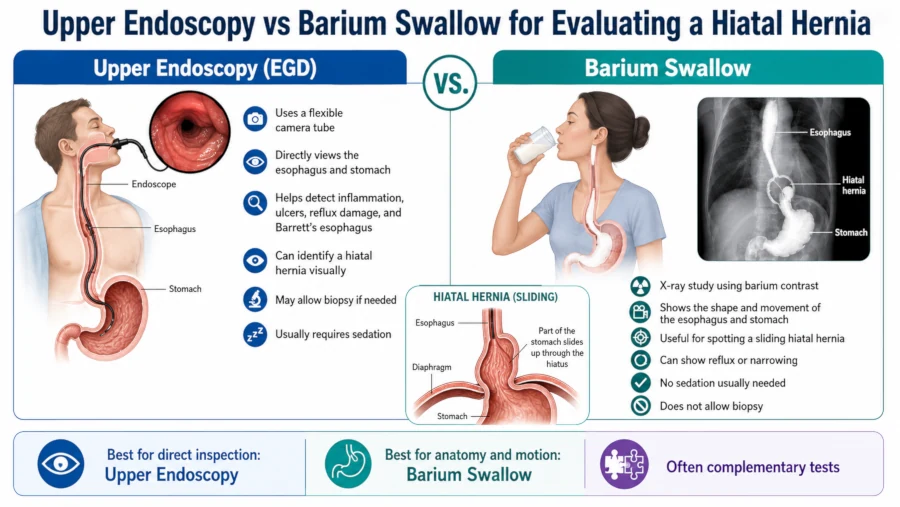
A hiatal hernia occurs when part of the stomach pushes upward through the diaphragm — the dome-shaped muscle that separates the chest cavity from the abdomen — and into the chest. The diaphragm has a small natural opening called the hiatus, which normally allows only the esophagus to pass through. When this opening widens or the surrounding tissue weakens, a portion of the stomach can slide or roll into the chest.
Most people with a small sliding hiatal hernia have no symptoms and discover the hernia incidentally during a procedure done for another reason. Larger hernias can produce heartburn, regurgitation, difficulty swallowing, chest pain, early fullness after meals, and, in severe cases, breathing problems.
Types of Hiatal Hernia
There are four recognised types, with Type I being by far the most common:
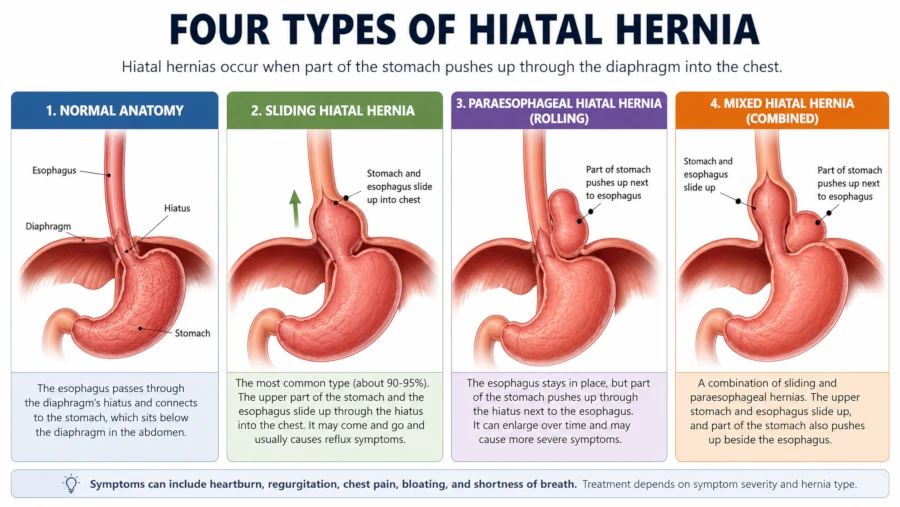
Types II–IV are collectively called paraesophageal hernias. They are less common but can cause more serious complications, including strangulation of the herniated stomach — a reason why large paraesophageal hernias are often referred for surgery even without symptoms.
Who Is at Higher Risk?
Risk factors for developing a hiatal hernia include:
- Age over 50 — prevalence rises from roughly 10% in adults under 40 to around 70% in those over 70, though only a fraction have symptoms [Mayo Clinic News Network, 2022]
- Obesity — excess abdominal pressure pushes against the diaphragm [Assakran et al., Cureus, 2021]
- Chronic coughing or heavy lifting — repeated strain can weaken the hiatus
- Smoking — associated with connective tissue changes that weaken the diaphragm
- Prior esophageal or gastric surgery
What Does Hiatal Hernia Endoscopy Detect?
An upper endoscopy (EGD) is recommended for all patients with suspected or confirmed symptomatic hiatal hernia because it provides direct visual information that other tests cannot match as comprehensively in one sitting. According to a review published in the Annals of Laparoscopic and Endoscopic Surgery, endoscopy serves several purposes:
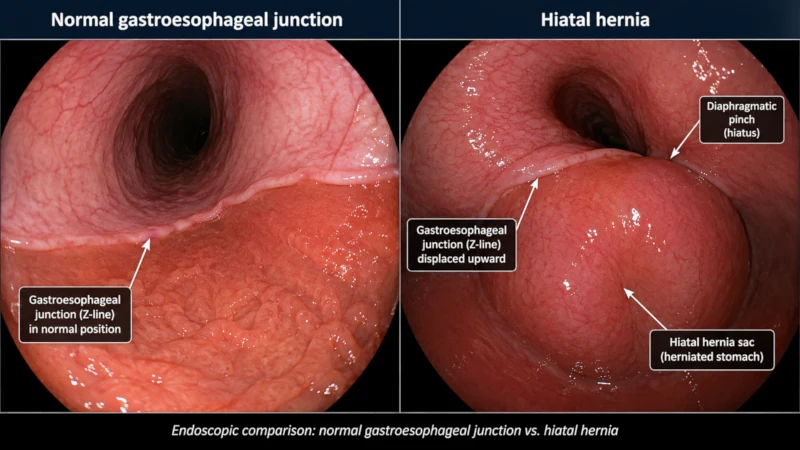
- Confirming the hernia — the endoscopist measures the distance between the esophagogastric junction (EGJ) and the diaphragmatic impression; a gap of more than 2 cm is considered diagnostic for a sliding hernia [Laracca, ALES, 2021]
- Assessing hernia size and type — the extent of gastric herniation is documented
- Identifying esophagitis — inflammation or ulceration caused by chronic acid reflux
- Detecting Barrett’s esophagus — a precancerous change in the esophageal lining that can develop from long-standing acid reflux
- Ruling out strictures — narrowing of the esophagus from scar tissue, which causes dysphagia
- Taking biopsies — tissue samples can identify Helicobacter pylori infection, Barrett’s changes, or other pathology
How Accurate Is Endoscopy for Diagnosing a Hiatal Hernia?
Endoscopy is highly specific for hiatal hernia — meaning that when it reports a hernia, the diagnosis is usually correct. However, its sensitivity (the ability to detect a hernia when one truly exists) is more variable, particularly for smaller hernias.
A multicenter retrospective study covering more than 162,000 upper endoscopies found a hiatal hernia detection rate of 24.4%, with rates rising sharply with age — from 16.5% in those under 50 to 37.3% in those over 80. Hernias were most often found in patients presenting with heartburn or reflux symptoms (38.7% of that group).
Note: Endoscopy can underestimate hernia size because the stomach position shifts with breathing and air insufflation during the procedure. When clinical or radiological findings conflict with endoscopy, a barium swallow study or high-resolution manometry may be added. High-resolution manometry has shown superior sensitivity and specificity in some comparison studies, though it is not universally required. [Tolone et al., PMC, 2018]
Endoscopy vs. Other Diagnostic Tests for Hiatal Hernia
Your doctor may use one or more of the following tests, often in combination:
| Test | What It Shows | Key Limitations |
| Upper endoscopy (EGD) | Direct mucosal view; biopsy capability; hernia type and size | Can miss small hernias; accuracy varies by endoscopist |
| Barium swallow (X-ray) | Hernia anatomy and size; swallowing mechanics | Radiation; no biopsy; less mucosal detail |
| CT scan | Large hernias and organ position; useful after prior surgery | Radiation; limited mucosal detail for small hernias |
| High-resolution manometry | Lower esophageal sphincter position relative to diaphragm; superior sensitivity | Specialist equipment; not universally available |
| pH monitoring (24-hr) | Acid exposure in the esophagus (GERD severity) | Does not diagnose hernia directly |
In practice, endoscopy is usually the first-line test. A barium swallow or CT scan may be added when the hernia is large, when anatomy is complex, or when surgery is being planned. Manometry and pH studies are added when GERD needs to be quantified.
Preparing for a Hiatal Hernia Endoscopy
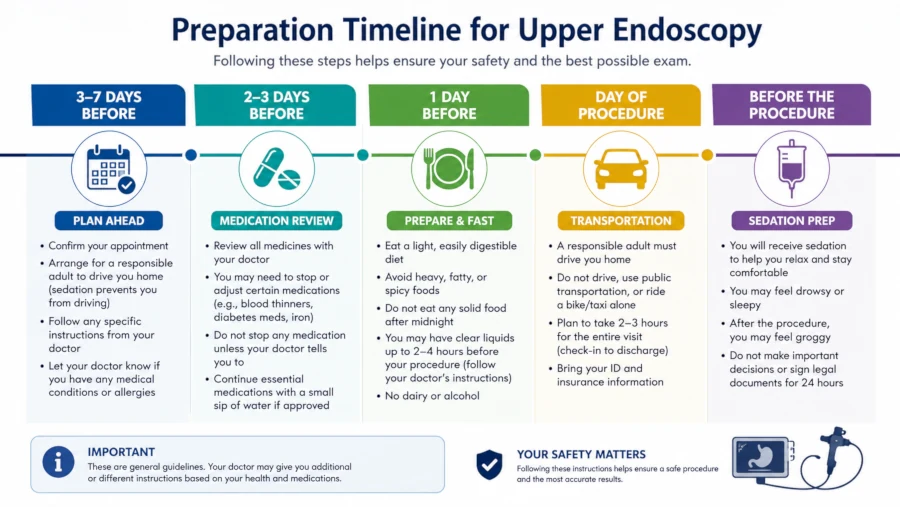
Preparation is straightforward but essential for safety and for getting a clear view of the esophagus and stomach. Your physician will give you specific instructions tailored to your health and the medications you take. General guidance from national gastroenterology bodies includes the following.
Fasting Before the Procedure
- Solid food: avoid for at least 6–8 hours before the procedure
- Clear liquids (water, black coffee without milk, clear tea): generally permitted up to 2 hours before, though specific guidelines vary by facility
- Always follow your endoscopy unit’s fasting instructions exactly — they may be stricter depending on your sedation plan
Medication Adjustments
Tell your doctor about every medication you take. Common adjustments include:
- Blood thinners (anticoagulants) such as warfarin, apixaban, or clopidogrel — these may need to be paused before the procedure, especially if a biopsy is planned. Do not stop them without explicit medical guidance.
- Aspirin — guidance varies; some physicians advise continuing low-dose aspirin
- Insulin and diabetes medications — dosing is usually adjusted because you will be fasting
- Iron supplements — often stopped 5–7 days before as they can coat the mucosa
Sedation Options
Most upper endoscopies in the United States are performed under conscious sedation (moderate sedation) or monitored anesthesia care (MAC). Some units offer unsedated procedures, which are shorter but less comfortable.
- Midazolam — induces relaxation and anterograde amnesia; commonly used for conscious sedation
- Fentanyl or other short-acting opioids — added for pain management
- Propofol — deeper sedation for more anxious patients or when therapeutic interventions are planned
You will need someone to drive you home if you receive sedation. Plan to avoid driving, operating machinery, and signing legal documents for the rest of the day.
What Happens During the Procedure — Step by Step
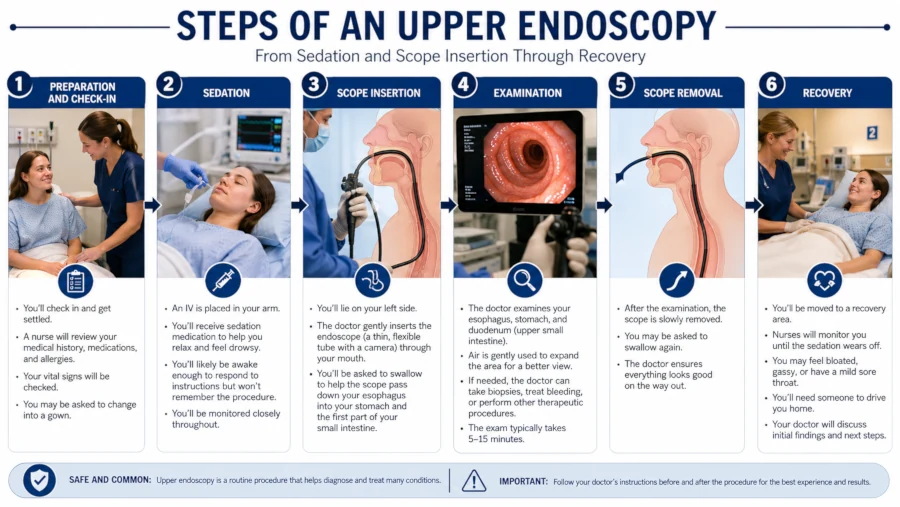
- Arrival and IV line placement. Staff record your vital signs (heart rate, blood pressure, oxygen level) and insert an intravenous line for sedation and any emergency medications.
- Throat spray. A topical anaesthetic spray may be applied to the back of your throat to reduce the gag reflex.
- Sedation. Medication is given through the IV line. Within minutes you will feel drowsy. Most people have no memory of the procedure itself.
- Bite block and positioning. A plastic bite block protects the endoscope and your teeth. You are positioned on your left side.
- Endoscope insertion. The endoscopist guides the thin, flexible tube (about 9–12 mm in diameter) gently through your mouth, past the throat, and into the esophagus and stomach. Air is insufflated to open the lumen for visibility.
- Examination. The gastroenterologist inspects the esophageal lining, the esophagogastric junction, and the stomach. The position and size of any hernia are documented. If the stomach is seen above the diaphragm during both forward-viewing and retroflexed (turned back toward the cardia) inspection, a hiatal hernia is confirmed.
- Biopsy (if needed). Small forceps through the endoscope’s working channel retrieve tiny tissue samples. This is painless.
- Scope removal and recovery. The endoscope is carefully withdrawn. You are monitored in a recovery area until you are alert and stable. The whole procedure typically takes 10–20 minutes, though you may be in the unit for 1–2 hours in total.
Safety and Complications
Upper endoscopy is among the most commonly performed gastrointestinal procedures and has a strong safety record. According to StatPearls (NCBI Bookshelf), major complications occur in fewer than 2% of EGDs.
Common and Minor After-Effects
- Sore or scratchy throat — from the scope passing through the pharynx; usually resolves within 1–2 days
- Bloating and gas — from air insufflated during the exam; passes within a few hours
- Mild nausea — occasionally from sedation
- Grogginess — from sedation; clears within hours
Rare but Serious Complications
- Bleeding — minor oozing at a biopsy site is relatively common and stops on its own. Significant bleeding is rare and more likely in patients on anticoagulants or with clotting problems.
- Perforation — a tear in the esophageal or gastric wall occurs in roughly 0.03% of diagnostic EGDs. Risk is higher in patients with esophageal strictures or Zenker’s diverticulum.
- Sedation-related cardiopulmonary events — the most common category of serious complications. Include transient low blood pressure, low oxygen saturation, or (rarely) cardiac events. Risk is higher in older patients and those with significant comorbidities.
- Infection — extremely rare when equipment is properly reprocessed
Red-Flag Symptoms After Endoscopy — Seek Immediate Care If You Notice:
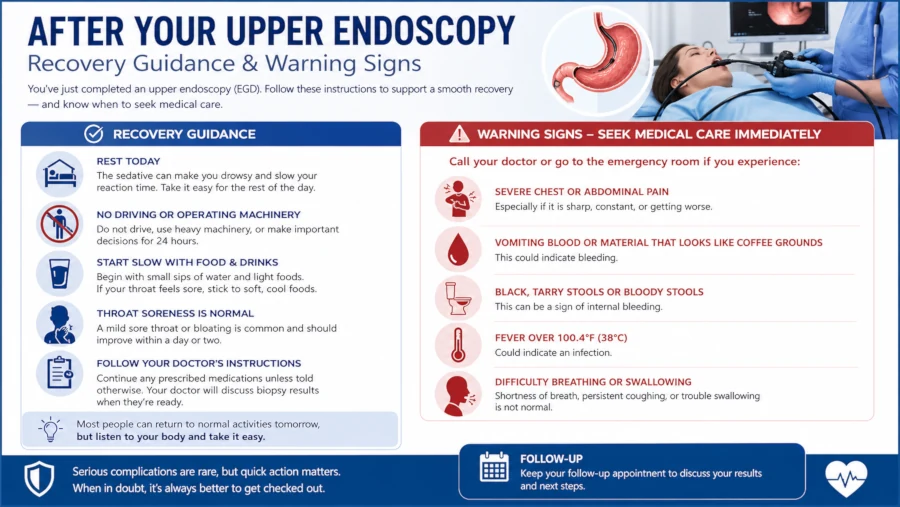
- Severe chest pain or abdominal pain
- Difficulty breathing or swallowing
- Bright red blood in stool or vomit, or black tarry stools
- Fever above 38°C (100.4°F)
- Neck stiffness or pain radiating to the back
Recovery and Post-Procedure Care
Immediately After
You will remain in the recovery area for 30–60 minutes while sedation wears off. A nurse will check your vital signs. You will usually receive a summary of the endoscopist’s initial findings before you leave. Formal biopsy results typically take 3–7 business days.
At Home — Days 1 and 2
- Throat discomfort: gargling with warm salt water and sucking on lozenges may help. Avoid smoking, alcohol, and highly acidic foods for 24 hours.
- Diet: start with soft, bland foods (soups, crackers, cooked vegetables, eggs) for the first day. Gradually return to your normal diet over 24–48 hours as tolerated.
- Activity: most people return to desk work and normal daily activity within 24 hours. Avoid strenuous exercise until the next day or as advised.
- Medications: resume your regular medications as instructed. If you were asked to stop blood thinners, confirm with your doctor when to restart them.
- Driving: do not drive for 24 hours after sedation.
What Happens After the Diagnosis?
The management of a hiatal hernia depends on its size, type, and whether it is causing symptoms or complications.
Lifestyle and Dietary Changes (Small Hernias, Mild Symptoms)
For most people with a small sliding hiatal hernia, lifestyle and dietary adjustments are the cornerstone of management:
- Eat smaller, more frequent meals
- Avoid eating within 2–3 hours of lying down
- Limit triggers such as fatty foods, caffeine, alcohol, spicy foods, chocolate, and citrus
- Elevate the head of the bed by 15–20 cm (6–8 inches)
- Maintain a healthy weight to reduce abdominal pressure
- Quit smoking
For more detail on foods to eat and avoid, see: Foods to Eat with Hiatal Hernia
Medications
- Antacids — neutralise stomach acid; useful for occasional heartburn relief
- H2 receptor blockers (e.g., famotidine) — reduce acid production; available over the counter
- Proton pump inhibitors (PPIs, e.g., omeprazole, pantoprazole) — most effective for controlling acid reflux; typically prescribed for symptomatic GERD associated with a hernia
Surgery
Surgery (usually laparoscopic fundoplication) is considered when symptoms are severe, do not respond to medications, or when a large paraesophageal hernia is present. For a full overview of when surgery is recommended, see: Hiatal Hernia Treatment Options
Reducing Your Risk of a Hiatal Hernia (or Its Worsening)
While hiatal hernias cannot always be prevented — age-related tissue changes play a role — several modifiable factors can reduce the risk or prevent an existing hernia from enlarging or becoming symptomatic:
- Maintain a healthy body weight — excess abdominal weight increases diaphragmatic pressure
- Avoid heavy lifting — or use correct technique and brace your core when lifting is unavoidable
- Treat chronic cough — address the underlying cause (asthma, post-nasal drip, ACE inhibitor use, smoking)
- Stop smoking — smoking weakens connective tissue throughout the body, including the diaphragm
- Avoid straining during bowel movements — treat constipation with diet, hydration, and fibre
| MEDICAL DISCLAIMER: This article is for informational and educational purposes only. It does not constitute medical advice and is not a substitute for professional diagnosis, treatment, or guidance from a qualified healthcare provider. If you have symptoms suggesting a hiatal hernia or any digestive condition, consult your doctor before making any changes to your care. |
Frequently Asked Questions
Will an endoscopy always show a hiatal hernia?
Not necessarily. Endoscopy is highly specific — if it finds a hernia, the diagnosis is reliable — but sensitivity is moderate. Small hernias can be missed if the stomach repositions during the exam. If symptoms strongly suggest a hiatal hernia but endoscopy is negative, a barium swallow or manometry may be ordered.
Is the procedure painful?
Sedation means that most patients have no memory of the procedure and feel no pain. You may experience a mild gag reflex as the scope passes your throat, and some throat soreness afterward, but significant pain during or after a diagnostic EGD is uncommon. Report severe pain to your doctor immediately.
How long does hiatal hernia endoscopy take?
The endoscopy itself usually takes 10–20 minutes. Including preparation, sedation, the procedure, and recovery monitoring, expect to be at the facility for 1.5 to 2.5 hours.
Can endoscopy treat a hiatal hernia, not just diagnose it?
Standard diagnostic endoscopy does not repair a hernia. There are experimental endoscopic repair techniques (such as mucosal ligation combined with clips) that have been reported in small case studies, but these are not standard practice. Surgical repair — typically laparoscopic fundoplication — remains the main treatment for symptomatic hernias that do not respond to lifestyle measures and medication.
When should I call my doctor after an endoscopy?
Contact your doctor promptly if you develop severe chest or abdominal pain, difficulty breathing or swallowing, high fever, or blood in your stool or vomit. These are rare but serious warning signs that need immediate evaluation.
Do I need a repeat endoscopy if I have a hiatal hernia?
This depends on what was found. If Barrett’s esophagus was identified, surveillance endoscopy is recommended at intervals determined by the degree of dysplasia found. If the initial scope was normal beyond the hernia, your gastroenterologist will advise whether and when follow-up is needed based on your symptom response to treatment.
References
- Mayo Clinic News Network (2022). Not Just a Hernia: Digging Deeper. → View source
- Mayo Clinic (2025). Hiatal Hernia — Diagnosis and Treatment. → View source
- Laracca G. Optimal workup for a hiatal hernia. Ann Laparosc Endosc Surg. 2021. → View source
- Bar-Yishay I, et al. Hiatal hernia: risk factors and clinical and endoscopic aspects in gastroscopy. PMC. 2024. → View source
- Tolone S, et al. High-resolution manometry is superior to endoscopy and radiology in assessing and grading sliding hiatal hernia. PMC. 2018. → View source
- Assakran BS, et al. Prevalence of asymptomatic hiatal hernia in obese patients during preoperative upper GI endoscopy. Cureus. 2021. → View source
- Bhutani MS. Esophagogastroduodenoscopy (EGD). StatPearls, NCBI Bookshelf. 2026. → View source
- American College of Gastroenterology (2025). Upper GI Endoscopy (EGD). → View source
- Johns Hopkins Medicine. Hiatal Hernia. → View source
- NIDDK. Chapter 24: Indications & Outcomes of Gastrointestinal Endoscopy. Burden of Digestive Diseases in the United States. → View source