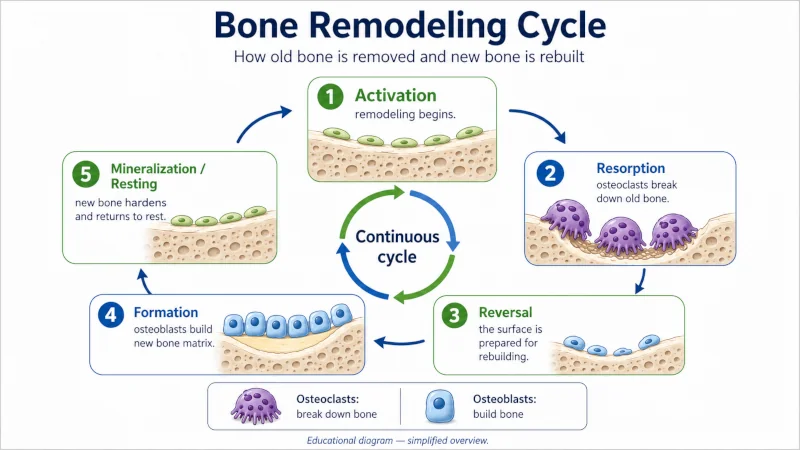
Foods for bone and muscle health do more than most people give them credit for. Your skeleton is living tissue — it breaks down and rebuilds itself in a continuous cycle called remodeling — and your muscle mass shifts over weeks and months depending on what you eat and how much you move. What lands on your plate either feeds that upkeep or slowly works against it.
This guide covers the foods with the strongest evidence behind them, the nutrients that matter most, and a few habits that may be quietly costing you bone and muscle. It is not a substitute for personal medical advice, especially if you have been diagnosed with osteoporosis, sarcopenia (age-related muscle loss), or a joint condition. For a wider look at the system these foods support, see our musculoskeletal health overview.

Why What You Eat Reaches Your Bones and Muscles
Bone, muscle, tendon, and cartilage all depend on a steady supply of specific nutrients. When those run short for long enough, your body takes what it needs from storage — and bone and muscle are where much of that storage sits. Calcium gets pulled out of bone to keep blood levels steady. Protein gets stripped from muscle when intake falls behind. Neither shows up overnight, which is exactly why diet is easy to neglect.
Food is one piece, not the whole picture. Genetics, hormones, physical activity, and certain medications all shape bone density and muscle strength. But your diet is the lever you reach for three times a day, and over decades it adds up.
The Nutrients That Matter Most
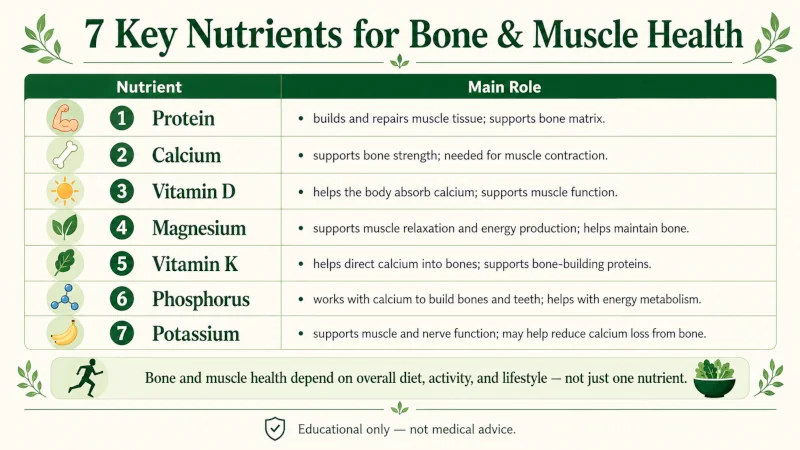
Seven nutrients carry most of the weight for bone and muscle. The table sums up what each one does and where to find it; the notes that follow add the detail that matters.
| Nutrient | Main role | Where to get it |
| Calcium | Chief mineral in bone; gives the skeleton its strength | Dairy, fortified plant milks, kale, bok choy, almonds, canned sardines |
| Vitamin D | Lets the gut absorb calcium; supports muscle and balance | Fatty fish, egg yolk, fortified foods, sunlight |
| Magnesium | Part of bone mineral; helps regulate vitamin D and calcium | Nuts, seeds, legumes, leafy greens, whole grains |
| Phosphorus | Pairs with calcium to form the hard mineral in bone | Meat, fish, dairy, legumes, nuts |
| Vitamin K | Activates osteocalcin, which binds calcium into bone | Leafy greens (K1); natto and fermented foods (K2) |
| Protein | Building material of muscle; also supports bone density | Meat, fish, dairy, eggs, legumes, soy |
| Vitamin C | Needed to make collagen, the framework of bone and cartilage | Citrus, bell peppers, kiwi, broccoli |
Calcium
About 99% of your body’s calcium is held in bones and teeth [NIH ODS, 2026]. When you don’t eat enough, your body borrows calcium from bone to keep blood levels stable, and over years that withdrawal thins the skeleton. The recommended intake is 1,000 mg a day for most adults, rising to 1,200 mg for women over 50 and men over 70 [NIH ODS, 2026].
Vitamin D
Without enough vitamin D, you absorb only a fraction of the calcium you eat, no matter how much that is. It also acts directly on muscle: low levels track with weakness and a higher fall risk in older adults [Holick, 2007] [NIH ODS, 2023]. Few foods carry much of it, which is why fortified products and sensible sun exposure matter.
Magnesium
Roughly 60% of the body’s magnesium sits in bone, and it helps steer both vitamin D metabolism and parathyroid hormone, which governs calcium [Castiglioni et al., 2013] [Rude et al., 2009]. Low intake tracks with lower bone density in population studies, though the evidence for supplements changing outcomes is mixed. Magnesium also drives normal muscle contraction — for more on what happens when it falls short, see what causes muscle cramps.
Phosphorus
Phosphorus joins calcium to build hydroxyapatite, the crystal that makes bone rigid. Most people in Western countries get plenty, so true deficiency is rare. The concern runs the other way: diets heavy in processed foods and cola, where phosphorus far outweighs calcium, may nudge bone metabolism in the wrong direction [Calvo & Uribarri, 2013].
Vitamin K
Vitamin K — especially K2 — helps switch on osteocalcin, the protein that locks calcium into the bone matrix. Reviews suggest K2 supplements may modestly improve bone density and lower fracture risk, but the evidence is rated moderate rather than settled [Cockayne et al., 2006] [Fusaro et al., 2017]. If you take a blood thinner such as warfarin, talk to your prescriber before changing your vitamin K intake.
Protein
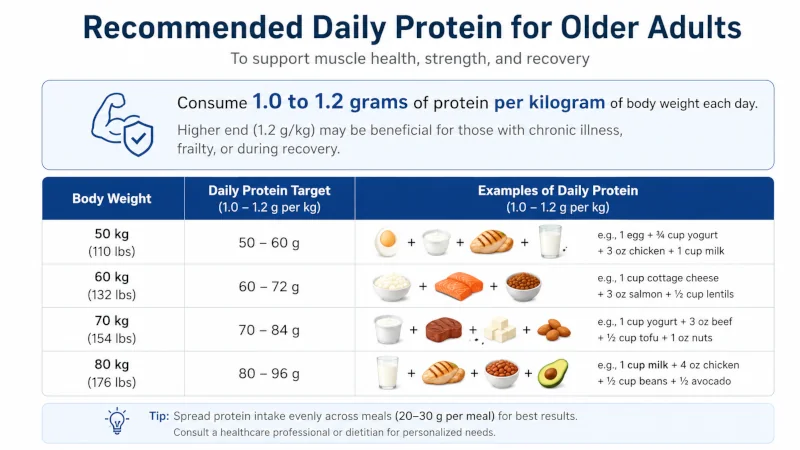
Protein is the raw material your body uses to build and repair muscle. Older adults generally do better on more of it — about 1.0 to 1.2 g per kilogram of body weight a day — to offset the muscle loss that comes with age [Bauer et al., 2013]. And contrary to an old worry, adequate protein supports bone rather than harming it, as long as calcium intake is sufficient [Kerstetter et al., 2011].
Vitamin C
Collagen is the main protein in bone matrix and cartilage, and your body can’t make it without vitamin C. Too little weakens connective tissue; adequate intake tracks with better bone density and lower fracture risk [Sahni et al., 2009].
The Best Foods for Bone and Muscle Health
No single food does everything. The strongest pattern is variety — several of these foods, most days, so the nutrients overlap and cover each other’s gaps.
Dairy and Fortified Alternatives
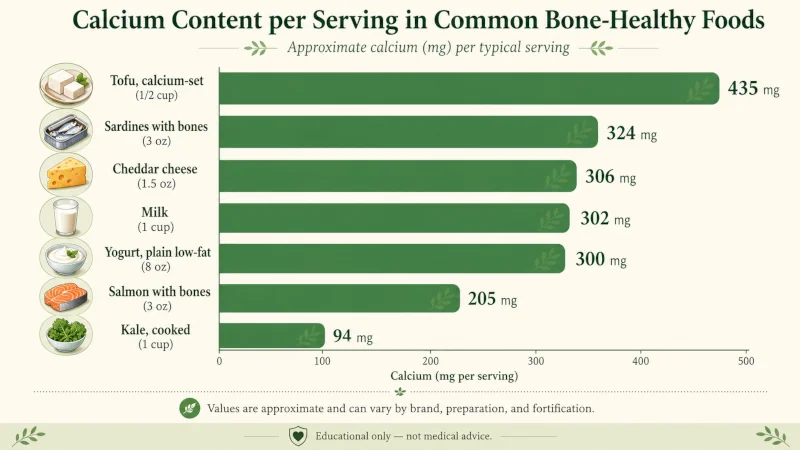
Milk, yogurt, and cheese pack calcium and protein together, and most are fortified with vitamin D. One cup of low-fat milk delivers about 300 mg of calcium — roughly a third of the adult daily target [USDA FoodData Central]. If you skip dairy, fortified oat, soy, almond, or rice milks can match those numbers, though how well the calcium absorbs varies by brand. Shake the carton; fortified calcium tends to settle.
Leafy Greens
Kale, bok choy, broccoli, and collard greens supply calcium, vitamin K1, and magnesium at once. The calcium in kale and bok choy actually absorbs as well as — or better than — the calcium in milk [Weaver et al., 1999]. Spinach and Swiss chard are the exception: they look calcium-rich on a label, but their oxalates bind most of it, so little gets through.
Nuts and Seeds
Almonds are among the better plant sources of calcium, magnesium, and phosphorus — a one-ounce serving (about 23 nuts) gives roughly 76 mg of calcium and 76 mg of magnesium [USDA FoodData Central]. Seeds pull their weight too: two tablespoons of sesame seeds add about 176 mg of calcium, and chia seeds are a close match.
Fatty Fish
Salmon, sardines, mackerel, and trout are some of the only foods that carry real vitamin D. Canned salmon and sardines eaten with their soft bones add calcium as well — about 180 to 200 mg in a 3-ounce serving of canned salmon [USDA FoodData Central]. The omega-3 fats in oily fish may help calm joint inflammation, though their direct effect on bone density is less clear [Weiler, 2016].
Legumes, Citrus, Eggs, and Fortified Foods
Beans, lentils, and chickpeas bring protein and magnesium with a little calcium, which makes them valuable for anyone eating little meat or dairy; soaking and cooking dried legumes cuts their phytates and frees up more of the minerals. Oranges, grapefruit, and kiwi cover vitamin C — the Framingham Osteoporosis Study linked higher vitamin C intake with greater bone density in older adults [Sahni et al., 2009]. Eggs add a modest dose of naturally occurring vitamin D along with protein and phosphorus. And fortified staples — orange juice, breakfast cereals, plant milks, some breads — count as legitimate sources, recognized as such by major health agencies [NIH ODS, 2026].
Foods and Habits That Work Against You
Diet runs in both directions. A handful of common patterns can speed up bone loss or muscle breakdown, though strength of evidence varies.
| Factor | Effect on bone or muscle | Evidence |
| Very high sodium intake | Raises the amount of calcium lost in urine | Moderate |
| Heavy alcohol use | Lowers bone formation; blunts muscle protein synthesis | Strong |
| Very high caffeine (>4 cups/day) | May slightly increase calcium excretion at high doses | Moderate |
| Heavy cola / soft-drink intake | Linked with lower bone density | Moderate (observational) |
| Very low protein intake | Impairs muscle repair; tied to higher fracture risk | Strong |
| Crash dieting / very low calories | Can drive rapid bone loss and muscle breakdown | Strong |
| Excess vitamin A from supplements | Linked with higher fracture risk at high doses | Moderate |
Context matters more than any single item. One cup of coffee does not cause osteoporosis. A decades-long pattern of too little calcium, low vitamin D, almost no weight-bearing exercise, and high sodium is what adds up.
What Changes With Age
Teens and Young Adults
The teenage years and early twenties are the build phase. As much as 90% of peak bone mass is in place by about age 18 in girls and 20 in boys [BHOF, 2023], which makes calcium, vitamin D, and overall nutrition during this window hard to make up later. Skimping here has lasting effects.
Adults Over 50
After peak bone mass, the job shifts from building to keeping. Calcium and vitamin D needs rise, protein becomes more important for holding onto muscle, and the single best-supported strategy is resistance exercise paired with enough protein [Cruz-Jentoft et al., 2019]. Staying steady on your feet matters just as much as bone density — our guide to fall prevention for older adults covers the rest.
After Menopause
Estrogen protects bone, so when it drops at menopause, bone loss speeds up — most sharply in the first several years. Calcium and vitamin D still matter, but food alone usually won’t hold off osteoporosis in someone with real risk factors. This is the point to talk with a clinician about bone-density screening and, in some cases, medication.
Claims That Run Ahead of the Evidence
A few foods get promoted with more confidence than the research supports. Here’s where the science actually stands.
Black currant. Lab and animal work has looked at its anti-inflammatory compounds, but human evidence for meaningful joint relief is thin. The popular comparison to the prescription drug indomethacin has not been shown in human trials.
Alfalfa sprouts. Alfalfa contains vitamin K and some minerals, yet human evidence for a specific bone benefit is early-stage. More to the point, raw sprouts are a recurring source of Salmonella and E. coli outbreaks, and the FDA advises that older adults, pregnant women, young children, and anyone immunocompromised avoid raw or lightly cooked sprouts entirely [FDA, 2024].
Coconut water. It offers potassium and a little magnesium, but the idea that it remineralizes bone or reverses osteoporosis has no clinical support.
The “alkaline diet.” The theory that acid-forming foods leach calcium from bone is plausible on paper but has not held up in controlled trials. Current consensus does not treat acid-alkaline balance as the main framework for a bone-healthy diet [Fenton et al., 2011].
When Food Alone Isn’t Enough
Nutrition is one part of bone and muscle health; it rarely works alone. Some situations call for a professional assessment rather than another serving of kale.
Talk with a healthcare provider if any of these apply to you:
- You have been diagnosed with osteoporosis or osteopenia.
- You are within the first 5 to 10 years after menopause.
- You take medication that affects bone — long-term corticosteroids, proton pump inhibitors, or anticonvulsants.
- You have a condition that limits nutrient absorption, such as Crohn’s disease, celiac disease, or a history of bariatric surgery.
- You have a family history of early fractures.
- You are over 65 and have fallen or feel unsteady.
Calcium and vitamin D supplements help many people who can’t reach their needs through food. One caveat: a few studies have tied high-dose calcium supplements to a possible rise in cardiovascular risk, though the evidence is debated and far from settled [Bolland et al., 2011]. For types, doses, and interactions, see our guide to calcium and vitamin D supplements. A simple blood test (25-hydroxyvitamin D) is the only reliable way to know whether you actually need vitamin D, since status swings with skin tone, age, sun exposure, and geography.
If joint pain rather than bone loss is the issue, an anti-inflammatory, Mediterranean-style way of eating may ease symptoms, but it supports treatment — it doesn’t replace it.
| Health Disclaimer: This article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a qualified healthcare provider before making significant changes to your diet, especially if you have a diagnosed condition, are pregnant or breastfeeding, or take medication. Do not use this information to self-diagnose or self-treat any medical condition. |
Frequently Asked Questions
Is dairy the only good source of calcium?
No. Kale and bok choy, almonds, fortified plant milks, canned fish with bones, beans, and fortified foods all add up. A well-planned diet meets calcium needs without any dairy at all.
Do I need a calcium supplement if I eat well?
Often not. Many people reach their needs through food. Whether a supplement helps depends on your total intake, your age, and any condition that affects absorption — a doctor or registered dietitian can help you work out the gap, if there is one.
Does eating more protein really help preserve muscle as I age?
Yes, based on current evidence. Older adults need more protein than younger adults to get the same muscle-building response, and spreading it across meals rather than loading one sitting appears to help.
Does coffee leach calcium from bones?
Only at high intakes — more than four to five cups a day — and even then the effect is small and easily offset by adequate calcium. For most moderate drinkers, coffee is not a meaningful driver of bone loss.
Can anti-inflammatory foods help joint pain?
A Mediterranean-style diet rich in omega-3s, polyphenols, and fiber has some evidence for lowering markers of inflammation. For conditions like rheumatoid arthritis it supports treatment rather than replacing it, so significant joint pain still needs a medical evaluation.
References
- NIH Office of Dietary Supplements. Calcium: Fact Sheet for Health Professionals. Updated 2026. → View source
- NIH Office of Dietary Supplements. Vitamin D: Fact Sheet for Health Professionals. Updated 2024. → View source
- NIH Office of Dietary Supplements. Magnesium: Fact Sheet for Health Professionals. → View source
- Holick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–281. → View source
- Castiglioni S, et al. Magnesium and osteoporosis: current state of knowledge. Nutrients. 2013;5(8):3022–3033. → View source
- Rude RK, Singer FR, Gruber HE. Skeletal and hormonal effects of magnesium deficiency. J Am Coll Nutr. 2009;28(2):131–141. → View source
- Calvo MS, Uribarri J. Public health impact of dietary phosphorus excess. Adv Nutr. 2013;4(5):542–553. → View source
- Cockayne S, et al. Vitamin K and the prevention of fractures. Arch Intern Med. 2006;166(12):1256–1261. → View source
- Fusaro M, et al. Vitamin K and bone. Clin Cases Miner Bone Metab. 2017;14(2):200–206. → View source
- Bauer J, et al. Evidence-based recommendations for optimal dietary protein intake in older people. JAMDA. 2013;14(8):542–559. → View source
- Kerstetter JE, Kenny AM, Insogna KL. Dietary protein and skeletal health. Curr Opin Lipidol. 2011;22(1):16–20. → View source
- Weaver CM, Proulx WR, Heaney R. Choices for achieving adequate dietary calcium with a vegetarian diet. Am J Clin Nutr. 1999;70(3):543S–548S. → View source
- Sahni S, et al. Protective effect of total and supplemental vitamin C intake on bone loss in elderly men and women. J Nutr / Osteoporos Int. 2009. → View source
- Weiler HA. Omega-3 fatty acids and bone health. Prostaglandins Other Lipid Mediat. 2016. → View source
- Fenton TR, et al. Causal assessment of dietary acid load and bone disease. Nutr J. 2011;10:41. → View source
- Cruz-Jentoft AJ, et al. Sarcopenia: revised European consensus on definition and diagnosis (EWGSOP2). Age Ageing. 2019;48(1):16–31. → View source
- Bolland MJ, et al. Calcium supplements with or without vitamin D and risk of cardiovascular events. BMJ. 2011;342:d2040. → View source
- U.S. FDA. Selecting and Serving Produce Safely. Updated 2024. → View source
- U.S. Department of Agriculture. FoodData Central. → View source
- Bone Health & Osteoporosis Foundation. bonehealthandosteoporosis.org. → View source