Contents
- 1 What the research actually shows
- 2 How isometric training lowers blood pressure
- 3 The handgrip protocol, step by step
- 4 The wall sit protocol, step by step
- 5 Handgrip vs wall sit: which to choose
- 6 Four mistakes that cancel out the benefit
- 7 How to track your response
- 8 Safety: who should pause and ask first
- 9 Realistic expectations
- 10 When to talk to a Doctor
- 11 Frequently asked questions
- 12 References

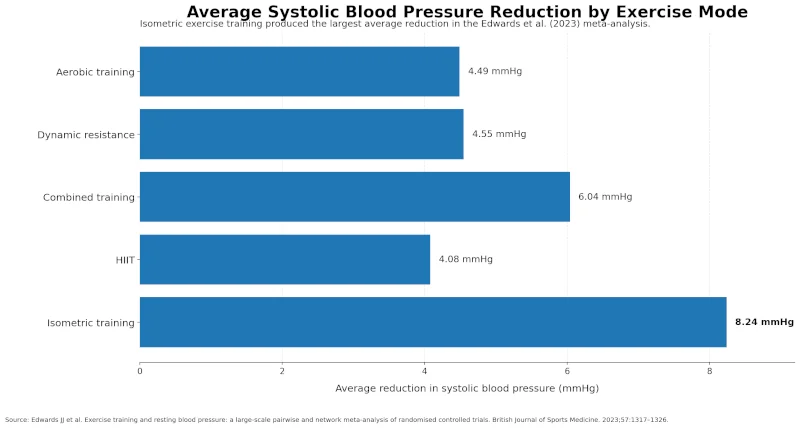
Isometric exercise for blood pressure is one of the most consistently effective non-drug ways to lower a resting reading, and the catch is that most people do it wrong. A 2023 network meta-analysis of 270 randomised trials and 15,827 adults compared every common exercise mode and ranked isometric training first, with average reductions of about 8.24 mmHg systolic and 4.00 mmHg diastolic — roughly double what aerobic training produced in the same analysis [BJSM, 2023].
Explore related products and helpful tools.
As an Amazon Associate I earn from qualifying purchases.
Two protocols carry almost all of that evidence: isometric handgrip squeezes and the wall sit. Both use the same dosing pattern — four 2-minute holds, three days a week, at a moderate (not maximal) effort. This guide walks through how to do each one, the four mistakes that wipe out the benefit, who should not try it, and how to tell if it is working. For broader context on movement and hypertension, see our overview of exercise for blood pressure.
What the research actually shows
Three lines of evidence support isometric training. The Edwards 2023 network meta-analysis ranked isometric exercise the most effective single mode for resting blood pressure reduction across 270 trials [BJSM, 2023]. An earlier Mayo Clinic Proceedings meta-analysis by Carlson and colleagues pooled randomised trials of isometric handgrip training specifically and reported a mean systolic drop of around 6.8 mmHg and diastolic drop of around 3.9 mmHg over 4–10 weeks of training [Carlson et al., 2014]. A 2018 hemodynamic safety study by Wiles and colleagues monitored 26 men with stage 1 hypertension through wall-squat sessions and recorded no systolic readings above 250 mmHg during any hold, supporting the safety of the standard protocol in well-screened adults with mildly elevated pressure [Wiles et al., 2018].
Two caveats matter. First, the meta-analyses pool trials that vary in length, intensity, and population — averages do not promise any individual reading will fall by a specific amount. Second, isometric training has been studied less in people with stage 2 hypertension, untreated severe hypertension, or significant heart disease, so existing evidence applies most directly to adults with elevated or stage 1 readings whose clinicians have cleared them to exercise.
How isometric training lowers blood pressure
During a sustained contraction, blood vessels supplying the working muscle are mechanically compressed and local blood flow drops. When the hold releases, blood rushes back through those vessels, and the resulting surge in shear stress prompts the endothelium — the inner lining of the vessel — to release nitric oxide and related vasodilators. Repeat that pattern three days a week, and the endothelium becomes more responsive over time, lowering total peripheral resistance [Carlson et al., 2014].
The effect builds slowly. Most trials report measurable resting drops between weeks 4 and 8 [BJSM, 2023]. You will not feel different after a single session. For more on the vessel-side mechanism, see our explainer on nitric oxide for blood pressure.
The handgrip protocol, step by step
Equipment
A handgrip dynamometer (around $25–$40) lets you measure your maximum squeeze and dose intensity precisely. A simple handgrip trainer also works. A rolled-up hand towel or a soft tennis ball can teach the pattern, but you sacrifice the ability to set intensity by number.
Find your training intensity
- Squeeze the device as hard as possible for 3–5 seconds. Note the peak reading — that is your maximal voluntary contraction (MVC).
- Multiply by 0.30 to 0.40. That is your training load.
- Example: a 100 lb max squeeze means holding at 30–40 lb. With no measuring device, aim for an effort you could maintain while holding a normal conversation [Wiles et al., 2010].
The 4 × 2 session
This is the dose used in most positive trials [Wiles et al., 2010]:
- Hold: squeeze at 30–40% MVC for 2 minutes
- Rest: release completely for 2–3 minutes
- Repeat: 4 holds total — alternate hands or stay with one, either works
- Frequency: 3 non-consecutive days per week
- Time horizon: expect 4–8 weeks before resting readings shift
Breathe steadily through every hold. Holding your breath (the Valsalva maneuver) spikes blood pressure sharply and removes the safety margin built into the protocol.
The wall sit protocol, step by step
Setup
- Stand with your back flat against a smooth wall.
- Walk your feet forward and slide down until your thighs reach a comfortable angle. Beginners should start higher than 90 degrees — a shallower squat is fine.
- Keep your knees stacked over your ankles, never out past your toes.
- Arms hang relaxed at your sides or fold across your chest.
The session
Same 4 × 2 pattern as the handgrip protocol, three days per week [Wiles et al., 2018]:
- Hold: 2 minutes in your chosen squat depth
- Rest: 2–3 minutes standing or walking slowly
- Repeat: 4 holds
If 2 minutes is too long
Start with 30-second holds at a shallow angle. Add 15 seconds to each hold every week until you reach 2 minutes. Three holds instead of four also counts — the goal is consistency, not collapse.
Common form errors
- Knees drifting inward — push them gently outward toward the small toe
- Feet too close to the wall — knees end up past your toes, stressing the joint
- Holding the breath — keep slow, steady nasal breathing
- Heels lifting — keep them flat
Handgrip vs wall sit: which to choose
| Feature | Isometric handgrip | Wall sit |
| What it is | Sustained squeeze of a gripper or device at moderate intensity | Static squat held against a wall |
| Best for | Limited mobility, knee or back issues, travel, working at a desk | People without knee problems who prefer leg-based work |
| Skip if you have | Severe hand arthritis or recent hand/wrist surgery | Patellar pain, knee instability, or balance problems |
| Equipment cost | $0–$40 (tennis ball to dynamometer) | $0 (a wall) |
| Average BP reduction reported | ~6.8/3.9 mmHg over 4–10 weeks | Comparable; smaller direct evidence base |
Both protocols use the same 4 × 2 dose and similar effect sizes. Pick the one you will actually do.

Four mistakes that cancel out the benefit
1. Squeezing or holding at maximum effort
The studied protocols use 30–40% of your max — not an all-out grip [Wiles et al., 2010]. Maximum effort spikes intra-arterial pressure during the hold and undermines the recovery-driven adaptation that does the work. Firm, not crushing.
2. Breath-holding
Closing the glottis under load (Valsalva) drives systolic pressure well above 200 mmHg in many adults. Steady breathing is non-negotiable. If you find yourself bracing, your intensity is too high — drop the load until you can breathe smoothly.
3. Doing it whenever you remember
Random squeezes in traffic do not produce the vascular adaptations seen in trials. Three structured sessions a week, with consistent timing and the full hold-rest pattern, is what the evidence supports [BJSM, 2023].
4. Not measuring before you start
If you have no baseline, you cannot tell if anything is working. Spend a week recording morning and evening readings on a validated home cuff before session one. Our guide on home blood pressure monitoring walks through the proper technique.
How to track your response
Treat the first week as a measurement-only week. Take two readings each morning and each evening, one minute apart, using the same arm, in a quiet room after five minutes of sitting. Average all the readings — that average, not any single number, is your baseline. Many readers find this is also when white-coat differences disappear, because home conditions are calmer than a clinic.
Once you start training, log every session and check your home average once a week. Track three columns: date, session completed (4/4 or fewer), and your weekly average. A simple example log:
| Date | Session | Weekly home average | Notes |
| Mon | Handgrip 4 × 2 | 134/86 | All four holds completed |
| Wed | Handgrip 4 × 2 | — | Stopped after 3 holds — light dizziness on hold 3 |
| Fri | Handgrip 4 × 2 | 132/84 | Smooth session |
| Mon (wk 2) | Handgrip 4 × 2 | — | Easy |
If your average falls by 3–8 mmHg systolic between weeks 4 and 8, you are responding within the range trials report [BJSM, 2023]. If readings have not budged by week 8, recheck technique and intensity before assuming you are a non-responder.
Safety: who should pause and ask first
Blood pressure rises during every isometric hold. That is expected — the therapeutic effect comes from the repeated rise-and-recovery cycle, not from training while already calm. The problem is starting from an unsafe baseline. Get clearance from your clinician before training if any of the following applies [ACSM]:
- Uncontrolled blood pressure (resting systolic above 160 mmHg or diastolic above 100 mmHg)
- History of heart attack, stroke, or heart failure within the past 6 months
- Known aortic aneurysm or aortic dissection
- Severe aortic stenosis or other significant valvular disease
- Proliferative retinopathy or recent eye surgery (intraocular pressure rises during holds)
- Pregnancy — isometric training is not well studied in pregnancy
- Implanted defibrillator or pacemaker with activity restrictions
Stop the session and call for help if you develop:
- Chest pain or tightness, or pain radiating to the jaw or left arm
- Sudden severe headache
- Lightheadedness, fainting, or near-fainting
- Blurred vision, double vision, or seeing spots
- Disproportionate shortness of breath
- Nausea or cold sweat during a hold
If you take blood pressure medication
Isometric training can lower readings further on top of medication. That is a benefit, but it is also why you should not change your dose on your own. Beta-blockers blunt heart rate responses to exercise, and some clinicians want to monitor readings closely before adjusting therapy. Bring your home log to your follow-up appointments [Whelton et al., 2018].
Realistic expectations
A few honest points to set up:
- Average reduction is modest, not dramatic. Pooled trials show roughly 6–8 mmHg systolic and 3–4 mmHg diastolic on average — meaningful for cardiovascular risk but not a substitute for medication when medication is indicated.
- Time to effect is weeks, not days. Plan to give it at least 8 weeks before judging the result.
- Adherence beats sophistication. A flawed handgrip routine you actually do for 12 weeks will beat a perfect wall-sit protocol you quit after week 3.
- It complements aerobic exercise. Current US guidelines still recommend regular aerobic activity for overall cardiovascular health [Whelton et al., 2018]. Many people add isometric training rather than replace walking or cycling.
When to talk to a Doctor
Book an appointment, do not wait for a routine visit, if:
- Your home average is consistently above 140/90 across two weeks
- Readings are climbing rather than falling after 4–6 weeks of consistent training
- You feel worse during or after sessions in a pattern that does not match normal muscle fatigue
- You start a new medication or your dose changes
Seek same-day care if you record a reading above 180/120 mmHg, especially with chest pain, severe headache, vision changes, shortness of breath, or new weakness.
| Health Disclaimer This article on isometric exercise for blood pressure is educational and is not medical advice. Isometric training raises blood pressure temporarily during each hold. If you have uncontrolled hypertension, heart disease, an aortic aneurysm, a recent stroke, retinopathy, are pregnant, or take blood pressure or heart medication, talk with your prescribing clinician before starting. Stop and seek care if you develop chest pain, severe headache, vision changes, fainting, or sudden shortness of breath. Do not stop or adjust prescribed medication based on home blood pressure readings without speaking to your clinician. |
Frequently asked questions
How long until I see results?
Most randomised trials report measurable changes between weeks 4 and 8 of consistent 3-day-per-week training [BJSM, 2023]. Track a weekly home average rather than reacting to single readings.
Can I do isometric training every day?
The dose tested in positive trials is 3 sessions per week with rest days between. Daily training has not been shown to add benefit and may interfere with the recovery-driven adaptation. Stick with three days.
Will this replace my blood pressure medication?
No. Average reductions are real but moderate. Some people reduce their medication under clinician supervision as readings improve, but stopping or adjusting medication on your own based on home readings is unsafe [Whelton et al., 2018].
Do I need a dynamometer?
It helps you dose intensity precisely, but a tennis ball or rolled towel is enough to learn the pattern. The protocol works as long as you avoid maximal effort and stay in the 30–40% MVC range — which a calibrated device makes easier to verify [Wiles et al., 2010].
What if my reading goes up rather than down?
Stop the protocol and consult your clinician. Common explanations are too much intensity, breath-holding during holds, an underlying condition that needs review, or simple individual variation. Continuing without sorting out the cause is not worth the risk.
Is wall sit or handgrip safer if I have hypertension?
Both have been studied in adults with stage 1 hypertension and show similar acute blood-pressure profiles when intensity is controlled [Wiles et al., 2018]. Pick based on your joints, not on perceived safety. If you have any cardiovascular condition, the clinician check comes first.
References
- Edwards JJ, Deenmamode AHP, Griffiths M, et al. Exercise training and resting blood pressure: a large-scale pairwise and network meta-analysis of randomised controlled trials. Br J Sports Med. 2023;57(20):1317–1326. doi:10.1136/bjsports-2022-106503. → View source
- Carlson DJ, Dieberg G, Hess NC, Millar PJ, Smart NA. Isometric exercise training for blood pressure management: a systematic review and meta-analysis. Mayo Clin Proc. 2014;89(3):327–334. doi:10.1016/j.mayocp.2013.10.030. → View source
- Wiles JD, Coleman DA, Swaine IL. The effects of performing isometric training at two exercise intensities in healthy young males. Eur J Appl Physiol. 2010;108(3):419–428. doi:10.1007/s00421-009-1025-6. → View source
- Wiles JD, Taylor K, Coleman D, Sharma R, O’Driscoll JM. The safety of isometric exercise: rethinking the exercise prescription paradigm for those with stage 1 hypertension. Medicine (Baltimore). 2018;97(10):e0105. doi:10.1097/MD.0000000000010105. → View source
- American College of Sports Medicine. Exercise for the Prevention and Treatment of Hypertension: Implications and Application. → View source
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. J Am Coll Cardiol. 2018;71(19):e127–e248. doi:10.1016/j.jacc.2017.11.006. → View source