You came home from the hospital with a folder of leaflets and a lot of contradictory advice. Here is the short version: the list of foods to avoid after a heart attack is shorter than most articles claim, and what you eat instead matters more than what you ban.
Five things carry most of the weight — processed and cured meat, salt, added sugar, saturated fat, and alcohol. Nearly everything else is a footnote. And there is one thing almost no list tells you: a few ordinary foods interfere with the medications you were almost certainly sent home with. Grapefruit is one. Potassium-based salt substitutes are the other, and that one is dangerous precisely because it looks like the healthy choice.
Foods to avoid after a heart attack: The short list
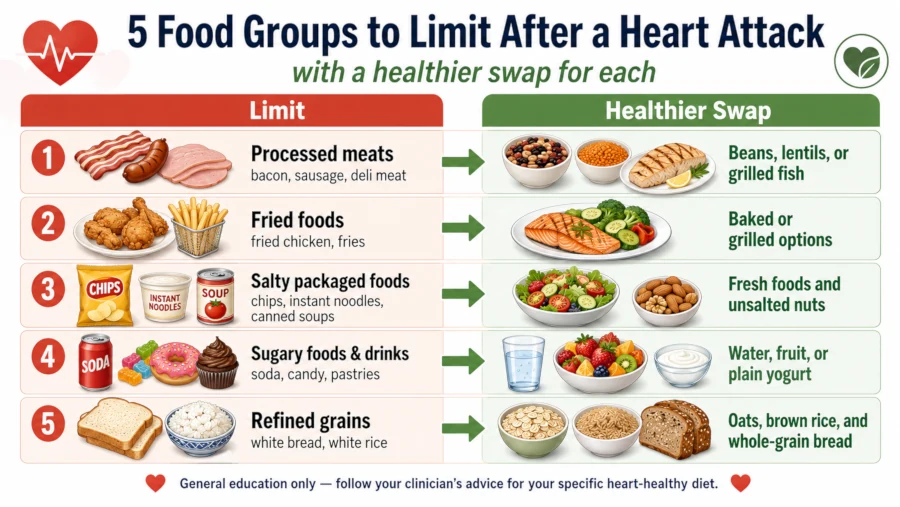
| Limit or avoid | Why it matters | A better move |
| Processed and cured meat | The clearest single food signal for coronary risk — heavy in salt and preservatives | Fish, beans, lentils, poultry, lean unprocessed cuts |
| Salt — mostly the hidden kind | Drives blood pressure, which drives a second event | Herbs, citrus, vinegar, garlic, pepper. Not potassium salt substitutes |
| Added sugar, especially in drinks | Raises triglycerides and body weight | Water, sparkling water, unsweetened tea |
| Saturated fat | Raises LDL cholesterol | Olive or canola oil, nuts, seeds, oily fish |
| Alcohol | Harm climbs steeply with the amount; interacts with your medications | Less, or none |
The swap is the active ingredient, not the ban
Cutting saturated fat works — but only depending on what fills the gap.
The best evidence here is a Cochrane review of 15 randomised trials in 56,675 adults. Reducing saturated fat for at least two years cut combined cardiovascular events by 17% (RR 0.83; 95% CI 0.70 to 0.98), rated moderate-quality evidence. For people who already had cardiovascular disease, 53 needed to make that change for about four years for one person to avoid an event they would otherwise have had [Cochrane review of saturated fat reduction, 2020].
Two honest caveats sit alongside that number. Reducing saturated fat had little or no effect on all-cause mortality. And the benefit came from replacement — swapping saturated fat for polyunsaturated fat or whole starchy foods. Trading butter for sugar buys you nothing.
That is the single most useful idea on this page. Every item below is really a swap.
Processed and cured meat

If you change one thing, change this. In a Circulation meta-analysis of 20 studies, each 50-gram daily serving of processed meat was associated with a 42% higher risk of coronary heart disease (RR 1.42; 95% CI 1.07 to 1.89). Unprocessed red meat, in the same analysis, showed no such association [Micha et al., Circulation, 2010].
The authors looked at why, and the answer is not what most people assume. Unprocessed and processed meats carried broadly similar saturated fat and cholesterol. What separated them was salt and nitrate preservatives.
Fifty grams is roughly two rashers of bacon, one hot dog, or a few slices of deli ham. That is not much. Bacon, salami, sausage, chorizo, corned beef, pâté, jerky, ham and most sliced sandwich meat all belong in the same bucket.
This is observational evidence, so it shows association rather than proof of cause. But it points the same direction as the American Heart Association’s 2021 dietary statement, which advises choosing lean, unprocessed cuts if you eat meat at all, and building most of your protein from plants, fish and low-fat dairy [AHA dietary guidance, 2021].
Salt, and where it is actually hiding
The AHA recommends no more than 2,300 mg of sodium a day, with an optimal goal of 1,500 mg for most adults. The average American eats over 3,300 mg. Cutting 1,000 mg a day is enough to improve blood pressure for most people [AHA sodium guidance, 2025].
The salt shaker is not your problem. More than 70% of the sodium people eat comes from packaged, prepared and restaurant food. Bread, deli meat, canned soup, pizza, sauces, cheese and takeout do the real damage, and none of them taste especially salty.

Read the sodium line on the label, check the serving size, and pick the lower option. That single habit will do more than any amount of restraint at the table. For more on the eating pattern that lowers blood pressure, see our guide to foods that lower blood pressure.
One warning before you reach for the obvious fix — see the medication section below. Do not switch to a potassium salt substitute without asking your doctor first.
Added sugar and sugary drinks
The AHA’s limits are 9 teaspoons (36 g) of added sugar a day for men and 6 teaspoons (25 g) for women. The average US adult eats about 17 teaspoons. Sugar-sweetened drinks are the largest single source, at roughly 24% of all added sugar [AHA added sugar guidance, 2024].
A single 12-ounce can of soda contains 10 teaspoons — more than a man’s entire daily allowance and nearly double a woman’s. Nothing else on this page can be fixed as quickly as that one.
Added sugar and alcohol are also the two biggest dietary drivers of high triglycerides, which is worth knowing if yours came back elevated; our guide to lowering triglycerides covers what actually works.
Saturated fat
Fatty and processed meat, butter, cream, full-fat cheese, coconut and palm oil, pastries and most commercial baked goods. The AHA’s guidance is to cook with liquid plant oils — olive, canola, sunflower — instead of tropical oils and hard fats [AHA dietary guidance, 2021].
Do not turn this into a low-fat crusade. The quality of fat matters more than the quantity. Olive oil, nuts, seeds, avocado and oily fish are not the enemy, and cutting them to replace the calories with white bread would be a step backwards.
Alcohol
This is the one place where the evidence is genuinely mixed, and you deserve the honest version rather than the comfortable one.
The AHA’s 2025 scientific statement on alcohol and cardiovascular disease found that at low intakes — no more than one to two drinks a day — the evidence ranges from no risk to possible risk reduction for coronary artery disease. The research is overwhelmingly observational, which means confounding is hard to rule out. At three or more drinks a day, or with binge drinking, the picture is not mixed at all: outcomes are consistently worse across every cardiovascular condition studied. The statement’s own conclusion is that it remains unknown whether drinking is part of a healthy lifestyle [AHA scientific statement on alcohol, 2025].
The World Health Organization takes a firmer line, stating that no level of alcohol consumption is safe for health. Both positions are defensible from the same data. That disagreement is the real answer.
What the AHA says in practice: if you don’t drink, don’t start. If you do drink, keep it low, and talk to your clinician — because alcohol interferes with a long list of medications, several of which you are probably taking now [AHA on alcohol and heart health].
Nobody credible is telling you to drink two glasses of wine a night for your heart.
Ultra-processed food and fried takeaway
The AHA’s 2021 statement asks for minimally processed foods over ultra-processed ones. The reason is simple arithmetic: ready meals, crisps, instant noodles, pastries and fast food deliver salt, sugar and saturated fat simultaneously, which is why they are so hard to fit into any of the limits above.
Frying deserves a specific correction. The old warning was that frying oils generate trans fats. That was really a story about partially hydrogenated oils — and the FDA determined in 2015 that these are no longer generally recognised as safe, barred manufacturers from adding them after June 2018, and set January 2021 as the final date for existing stock to clear distribution [FDA final determination on partially hydrogenated oils]. Ordinary frying oil is no longer a meaningful source of artificial trans fat in the US. The problem with fried takeaway is more ordinary than that: calories, salt, and whatever is being fried.
Four things you’ll be told to avoid that the evidence doesn’t support
Plenty of “cardiac diet” lists have not been updated in twenty years. These four come up constantly.
Margarine. The case against margarine was built on partially hydrogenated oil, which is essentially gone from the US food supply [FDA, 2015–2021]. Modern soft tub spreads made from liquid plant oils are the kind of fat current AHA guidance actively points you toward. Check the label for “partially hydrogenated” — it should not be there — and glance at the sodium.
Milk and dairy. The 2021 AHA statement lists low-fat and fat-free dairy among the healthy protein sources, not among the things to cut [AHA dietary guidance, 2021]. Butter and full-fat cheese are worth limiting because they are concentrated saturated fat. Skim milk and plain yogurt are not the same food, and blanket advice to avoid all dairy is not current guidance.
Unprocessed red meat. As above, the meta-analysis that found a 42% higher coronary risk with processed meat found no such association with unprocessed red meat [Micha et al., 2010]. That does not make steak a health food — the AHA still wants your protein to come mostly from plants — but the case against a lean cut of beef is far weaker than the case against bacon. (The separate WHO/IARC classification of red meat as “probably carcinogenic” concerns colorectal cancer, not heart disease [IARC Q&A, 2015]. Different question, different evidence.)
Eggs. The 2021 AHA statement does not single eggs out. It frames protein around choosing mostly plants, plus regular fish, low-fat dairy, and lean unprocessed meat. If you have high LDL cholesterol or diabetes, ask your clinician about your own limit rather than following a blanket number from a leaflet.
The food–medication interactions that actually matter
You probably left hospital on a statin, an antiplatelet such as aspirin or clopidogrel, a beta blocker, and often an ACE inhibitor or ARB. Some people also get spironolactone or an anticoagulant. Four food interactions are worth knowing by name.
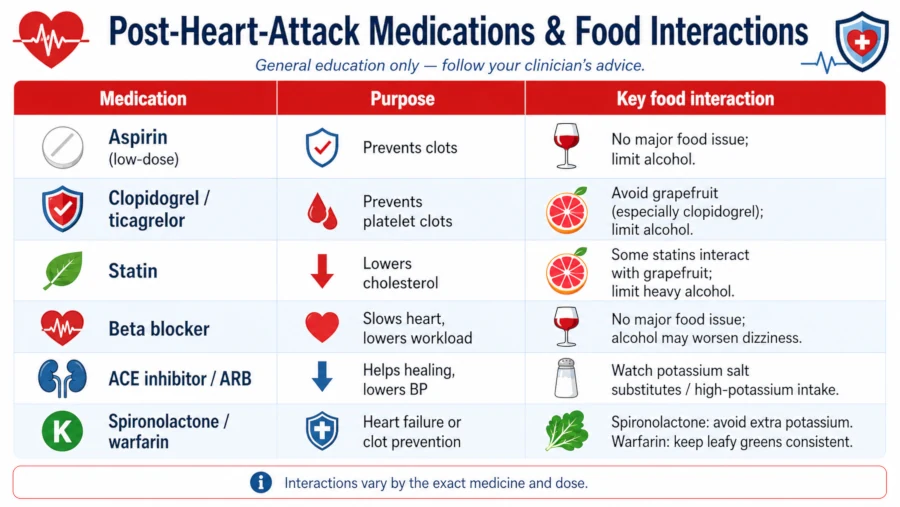
Grapefruit — statins and some heart-rhythm drugs. Grapefruit blocks an intestinal enzyme (CYP3A4) that normally breaks certain drugs down, so more of the drug reaches your bloodstream. The FDA names simvastatin (Zocor) and atorvastatin (Lipitor) among statins, nifedipine among blood-pressure drugs, and amiodarone among heart-rhythm drugs. With statins, too much drug in the body raises the risk of liver and muscle damage that can progress to kidney failure. Seville oranges, pomelos and tangelos can do the same thing [FDA on grapefruit and drug interactions]. Not every drug in these classes is affected — ask your pharmacist about yours by name.
Potassium salt substitutes — ACE inhibitors, ARBs and spironolactone. This is the one that catches people, because it arrives disguised as good behaviour. “Lite salt” and most salt substitutes are potassium chloride. ACE inhibitors (lisinopril, ramipril), ARBs (losartan, valsartan) and spironolactone all reduce your ability to clear potassium — that is part of how they work, not a fault. Stack potassium on top and levels can climb.
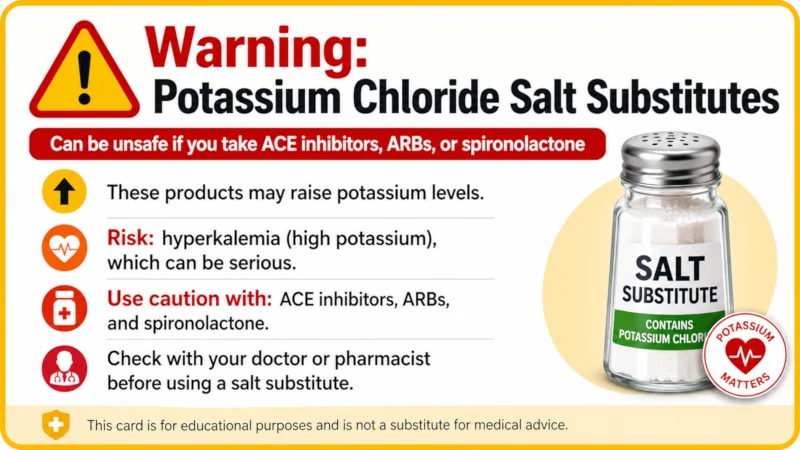
The FDA-approved labelling for lisinopril instructs prescribers to tell patients not to use potassium-containing salt substitutes without consulting their physician, and warns that high potassium can cause serious, sometimes fatal arrhythmias [FDA lisinopril label]. Spironolactone’s label carries the same warning [FDA Aldactone label, 2025]. Rising potassium usually causes no symptoms at all until it causes a rhythm problem.
Season with herbs, citrus, vinegar, garlic, pepper and chilli instead, and read the ingredients list for “potassium chloride” or “KCl.”
Vitamin K — warfarin. If you were sent home on warfarin, leafy greens are not forbidden. Sudden swings are the problem. Keep your intake roughly steady from week to week rather than avoiding greens, and tell your anticoagulation clinic before making a big dietary change [Mayo Clinic on the warfarin diet].
Alcohol — most of the above. Alcohol interacts with a long list of cardiac medications. This is a conversation to have with your pharmacist, not one to work out yourself.
What diet can and cannot do
Food is one lever. It is not the biggest one.
The single most effective thing available to you right now is cardiac rehabilitation — a supervised programme combining exercise training, education, and counselling to manage stress [AHA on cardiac rehab]. You should have received a referral when you were discharged; if you didn’t, ask your cardiologist or GP for one [AHA: Life After a Heart Attack].
Keep taking your medication. A cleaner diet is not a reason to stop a statin or a beta blocker, and no food on any list will do what those drugs do. Blood pressure and cholesterol respond to dietary change over weeks to months; the reduction in your risk of another event accumulates over years. Both things are true, and neither replaces the other.
If you want the positive version of this page — what to build meals around rather than what to cut — start with our guide to a heart-healthy diet. It is also worth getting your lipids rechecked on the schedule your cardiologist sets; our explainer on cholesterol testing covers what the numbers mean and where home kits fall short.
Who needs individual advice, not a list
General guidance stops being safe at a certain point. Ask for a referral to a registered dietitian if any of these apply:
- Heart failure. Your fluid and sodium targets are set for you personally and may differ from the numbers above.
- Chronic kidney disease. Potassium and protein targets change entirely, and high-potassium foods can become unsafe.
- Diabetes. Carbohydrate and cardiovascular targets need to be managed together.
- Warfarin. Vitamin K intake needs to be consistent, and changes need monitoring.
- Pregnancy or breastfeeding. Heart attack during pregnancy or the weeks after delivery is uncommon but real. Nutritional needs are different, alcohol should be avoided entirely, and this is not a situation for self-directed dieting or supplements — you need a cardiologist and a dietitian working together.
- Several medications at once. Bring the full list to your pharmacist and ask specifically about food interactions.
Red flags: when to call 911
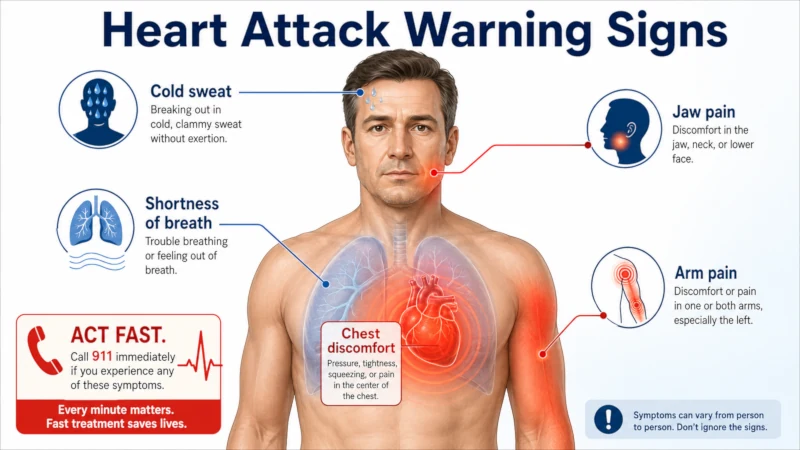
Do not wait to see whether it passes. Call emergency services immediately if you have:
- Chest discomfort — pressure, squeezing, fullness or pain — lasting more than a few minutes, or going away and coming back
- Discomfort in one or both arms, the back, neck, jaw or stomach
- Shortness of breath, with or without chest discomfort
- Cold sweat, nausea, or lightheadedness
Symptoms can be subtler in women, older adults and people with diabetes — shortness of breath, nausea, and back or jaw pain are more common. Do not drive yourself [AHA warning signs of a heart attack].
| Health Disclaimer: This article is for general education and information only. It is not medical advice and is not a substitute for diagnosis, treatment or guidance from a qualified healthcare professional. Recovery after a heart attack is individual: your sodium, potassium, fluid and medication targets are set by your care team, and they take priority over any general guidance here. Do not start, stop or change any medication, supplement, or salt substitute based on this page. If you are pregnant, breastfeeding, have kidney disease or heart failure, or take prescription medication, speak with your doctor or pharmacist before making dietary changes. If you think you may be having a heart attack, call your local emergency number immediately. |
Frequently Asked Questions
How strict do I need to be?
Consistency beats perfection. The evidence above describes patterns sustained over years, not a flawless week. One slice of birthday cake will not undo your recovery; bacon four mornings a week, quietly, for a decade, is the thing that adds up.
Can I ever eat bacon again?
Occasionally, yes. The risk described above is a dose–response relationship — it climbs with how much and how often, and there is no evidence that a rare rasher erases your progress. What you want to change is the default: bacon as a treat rather than a weekly habit.
Should I use a salt substitute?
Ask your doctor first, and do not assume it is safe. Most are potassium chloride, and if you take an ACE inhibitor, an ARB or spironolactone, the FDA labelling for those drugs specifically warns against potassium-containing salt substitutes without medical supervision [FDA lisinopril label]. Herbs, citrus, vinegar and spice blends do the same job with none of the risk.
Is red wine good for my heart?
No major health body recommends drinking alcohol for heart benefits. The 2025 AHA scientific statement concluded it remains unknown whether low-level drinking is part of a healthy lifestyle, while the WHO’s position is that no amount is safe [AHA scientific statement on alcohol, 2025]. If you already drink, keep it minimal and check with your pharmacist about your medications. If you don’t drink, there is no cardiac reason to start.
Will changing my diet prevent a second heart attack?
It lowers your risk; it does not eliminate it. In the Cochrane trials, 53 people with existing cardiovascular disease needed to reduce saturated fat over roughly four years for one to avoid an event [Cochrane, 2020]. That is a genuine benefit, and it is also why diet works best stacked with cardiac rehab, medication and not smoking — rather than instead of them.
How soon should I make these changes?
You can start with the drinks and the deli counter this week. Everything else is a gradual rebuild, and cardiac rehab is designed to walk you through it with a dietitian involved.
References
- Lichtenstein AH, Appel LJ, Vadiveloo M, et al. “2021 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association.” Circulation, 2021. doi:10.1161/CIR.0000000000001031. → View source
- Hooper L, Martin N, Jimoh OF, Kirk C, Foster E, Abdelhamid AS. “Reduction in saturated fat intake for cardiovascular disease.” Cochrane Database of Systematic Reviews, 2020, Issue 8. Art. No.: CD011737. doi:10.1002/14651858.CD011737.pub3. → View source
- Micha R, Wallace SK, Mozaffarian D. “Red and Processed Meat Consumption and Risk of Incident Coronary Heart Disease, Stroke, and Diabetes Mellitus: A Systematic Review and Meta-Analysis.” Circulation, 2010;121:2271–2283. doi:10.1161/CIRCULATIONAHA.109.924977. PMID 20479151. → View source
- Piano MR, Marcus GM, Aycock DM, et al. “Alcohol Use and Cardiovascular Disease: A Scientific Statement From the American Heart Association.” Circulation, 2025;152(1):e7–e21. doi:10.1161/CIR.0000000000001341. → View source
- American Heart Association. “Is drinking alcohol part of a healthy lifestyle?” heart.org. → View source
- American Heart Association. “How Much Sodium Should I Eat Per Day?” heart.org. Last reviewed July 2025. → View source
- American Heart Association. “How Much Sugar Is Too Much?” heart.org. Last reviewed September 2024. → View source
- U.S. Food and Drug Administration. “Final Determination Regarding Partially Hydrogenated Oils (Removing Trans Fat).” FDA, current as of October 2024. → View source
- U.S. Food and Drug Administration. “Grapefruit Juice and Some Drugs Don’t Mix.” FDA Consumer Updates. → View source
- DailyMed / U.S. National Library of Medicine. “Label: LISINOPRIL tablet” — Precautions, Information for Patients: Hyperkalemia. → View source
- U.S. Food and Drug Administration. “ALDACTONE (spironolactone) tablets — Full Prescribing Information,” Warnings and Precautions 5.1 (Hyperkalemia), 2025 label. → View source
- Mayo Clinic. “Warfarin diet: What foods should I avoid?” Expert answers. → View source
- American Heart Association. “Warning Signs of a Heart Attack.” heart.org. → View source
- American Heart Association. “Life After a Heart Attack.” heart.org. → View source
- American Heart Association. “What is Cardiac Rehabilitation?” heart.org. → View source
- International Agency for Research on Cancer (WHO). “Q&A on the carcinogenicity of the consumption of red meat and processed meat,” Monographs Volume 114. → View source