If your blood pressure won’t settle no matter what you change, the missing piece may not be your diet or your medication — it may be what happens after you fall asleep. Sleep and blood pressure are wired together: a healthy night lets your pressure fall, your heart rate slow, and your stress hormones reset. When sleep is short, broken, or interrupted by breathing problems, that nightly recovery doesn’t happen, and the strain shows up in your numbers.
The good news is that the connection between sleep and blood pressure runs both ways, and several of the fixes work quickly. This guide explains what your body is supposed to do overnight, the specific ways poor sleep pushes readings up, and a practical two-week plan to find — and change — your own pattern. The changes that tend to help fastest come first.
What Your Blood Pressure Does While You Sleep
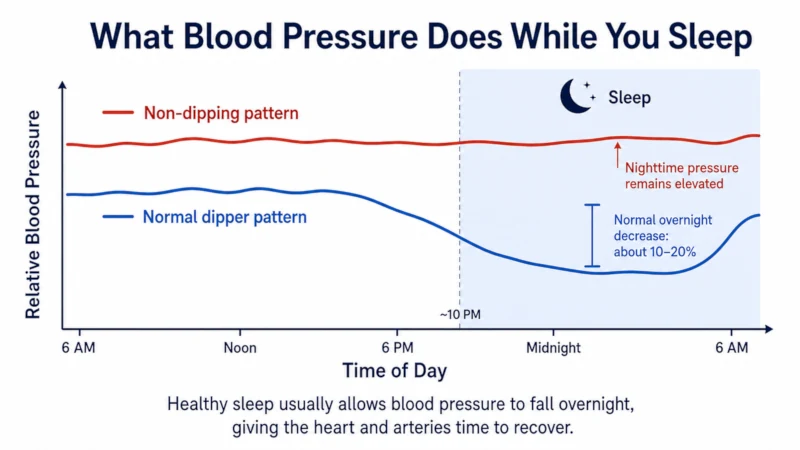
Blood pressure isn’t a fixed number. It follows a daily rhythm, and in healthy sleep it drops during the night as your nervous system winds down and blood vessels relax [American College of Cardiology, 2025]. Doctors call a nighttime fall of roughly 10–20% below your daytime average a normal “dipper” pattern. That overnight dip is thought to give your heart and arteries a genuine rest.
When that fall doesn’t happen — a “non-dipper” pattern, where nighttime pressure stays close to daytime levels — the risk picture changes. In a pooled analysis of more than 17,000 people with high blood pressure, a smaller nighttime dip was linked to more cardiovascular events, independent of the 24-hour average [Salles ABC-H meta-analysis, 2016]. Abnormally high pressure during sleep has been tied to greater risk of heart disease and stroke even when daytime readings look fine [American Heart Association, 2020].
What this means for you: you can’t see your overnight dip on a home monitor, but you can catch its shadow. If your morning readings run consistently higher than your evening readings, or you wake unrefreshed after a full night in bed, something may be interrupting that nightly fall. The rest of this guide is about finding what.
How Poor Sleep Pushes Blood Pressure Up
Short and disrupted sleep don’t raise blood pressure through a single mechanism. Too little sleep keeps stress hormones and the “fight or flight” nervous system switched on, and over time that’s associated with higher pressure. In a meta-analysis of adults, habitually short sleep was linked to roughly a 20% higher rate of existing high blood pressure and about a 33% higher risk of developing it in people under 65 [Wang meta-analysis, 2012]. These are associations, not proof that short sleep alone causes hypertension — but the direction is consistent across studies, and experimental sleep restriction does raise blood pressure [review in Current Hypertension Reports, 2023].
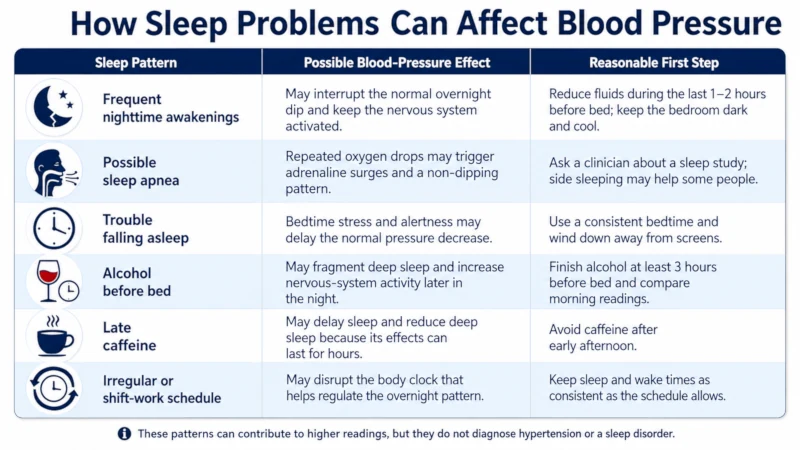
Quality matters, not just hours. Six fragmented hours are not the same as six consolidated ones. Frequent awakenings, reduced deep sleep, and breathing interruptions can all blunt the overnight dip even when total sleep time looks adequate. The table below shows the most common sleep patterns that affect blood pressure and a sensible first step for each.
| Sleep problem | How it can affect blood pressure | A reasonable first step |
| Frequent nighttime awakenings | Interrupts the overnight dip; keeps the nervous system activated | Cut fluids in the last 1–2 hours before bed; keep the room dark and cool |
| Suspected sleep apnea | Repeated drops in oxygen trigger adrenaline surges and a non-dipping pattern | Ask a clinician about a sleep study; try sleeping on your side |
| Trouble falling asleep (insomnia) | Elevated stress hormones at bedtime delay the pressure drop | Set a consistent bedtime; wind down away from screens |
| Alcohol before bed | Fragments deep sleep and raises sympathetic activity later in the night | Stop alcohol at least 3 hours before bed and compare your readings |
| Late caffeine | Delays sleep onset and shortens deep sleep | Avoid caffeine after early afternoon; its effect lingers for hours |
| Shift work / irregular schedule | Disrupts the circadian rhythm that governs the overnight pattern | Anchor sleep and wake times as consistently as your schedule allows |
Rotating night-shift work deserves a specific mention: over many years it has been associated with a modest but real increase in coronary heart disease risk in large studies of nurses [Vetter, JAMA, 2016]. If your schedule is flipped, standard “morning surge” advice tied to the clock won’t map onto your body — track your readings relative to your own sleep and wake times instead.
Sleep Apnea: The Cause That’s Most Often Missed
Of all the sleep problems that drive blood pressure up, obstructive sleep apnea (OSA) is the one most likely to be overlooked — partly because it happens while you’re unconscious. In OSA, the airway repeatedly narrows or closes during sleep, oxygen dips, and your body responds with surges of adrenaline that tighten blood vessels overnight.
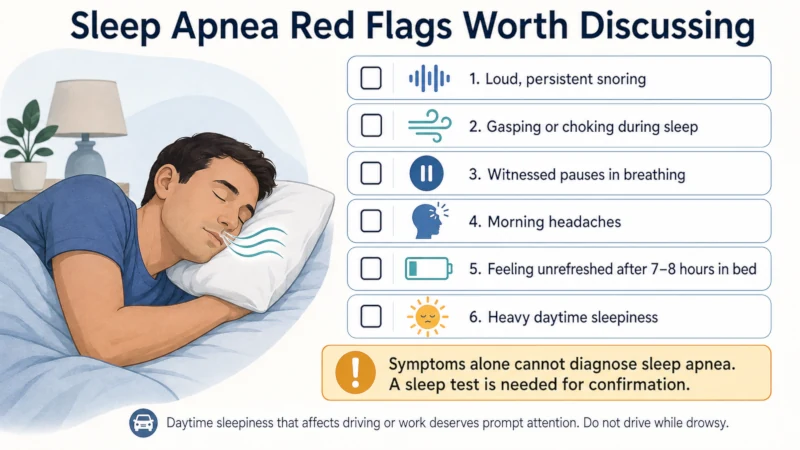
The link is strong in people whose pressure resists treatment. In a classic study of adults whose blood pressure stayed high despite multiple medications, about 83% turned out to have OSA [Logan, 2001]; across studies, estimates for resistant hypertension commonly run from roughly 60% to 90%. Red flags worth taking seriously include loud snoring with gasping or witnessed pauses in breathing, morning headaches, waking unrefreshed after 7–8 hours, and heavy daytime sleepiness. You can’t diagnose apnea from symptoms alone — that needs a sleep test — but these signs are a reason to ask for one.
Does treating it lower blood pressure? Honestly, modestly on average — and more if you use treatment consistently. In unselected patients, CPAP (continuous positive airway pressure) tends to lower pressure by only a few points. But in people with resistant hypertension and OSA, the effect is larger: pooled trials put the average 24-hour systolic reduction in the range of about 5–6 mmHg, with bigger drops in those who wear the mask reliably [CPAP resistant-hypertension meta-analysis, 2024]. So CPAP isn’t a replacement for blood pressure medication for most people, but for the right person it treats a real underlying driver. For the full picture, see our companion guide on sleep apnea and high blood pressure.
What Actually Helps — Starting With the Fastest Wins
You don’t need to overhaul your life at once. Change one thing at a time, keep tracking, and you’ll learn what your own body responds to. These are ordered roughly from fastest-acting to most involved.
- Move alcohol away from bedtime. Even a drink or two fragments deep sleep and raises nervous-system activity in the second half of the night. Stopping alcohol at least three hours before bed — or trialing a few alcohol-free weeks — is one of the changes people notice fastest.
- Dim the lights and put down screens before bed. Bright and blue-toned light in the last hour suppresses melatonin, which helps regulate both sleep and the overnight pressure pattern. Warmer, lower lighting in the evening supports the wind-down.
- Keep caffeine to the earlier part of the day. Caffeine’s effect lingers for about five to six hours on average — and much longer in some people — so an afternoon coffee can still be trimming your deep sleep at bedtime.
- Go lighter on salt in the evening. A very salty dinner promotes overnight fluid retention, which can nudge nighttime pressure up. General guidance from the American Heart Association is to work toward less than 2,300 mg of sodium a day, ideally closer to 1,500 mg for many adults — shifting some of that away from your last meal is a reasonable experiment.
- Keep the bedroom cool and dark. Many sleep specialists suggest a bedroom around 65–68°F (about 18–20°C). Too warm a room tends to fragment deep sleep.
- Anchor a consistent bedtime. Your circadian clock runs on predictability. A bedtime that stays within about a 30-minute window — even on weekends — supports a healthier overnight pattern.
- Add a short wind-down routine. Ten quiet minutes of slow breathing (in for 4 counts, out for 6), gentle stretching, or writing tomorrow’s worries onto paper can lower the bedtime stress response.
- Keep moving during the day. Regular exercise lowers resting blood pressure by a few points on average, with larger effects in people who start higher [Cornelissen & Smart, 2013]. Keep vigorous workouts out of the last couple of hours before bed, when they can delay sleep. See our guide to exercise for blood pressure.
A night-routine cheat sheet
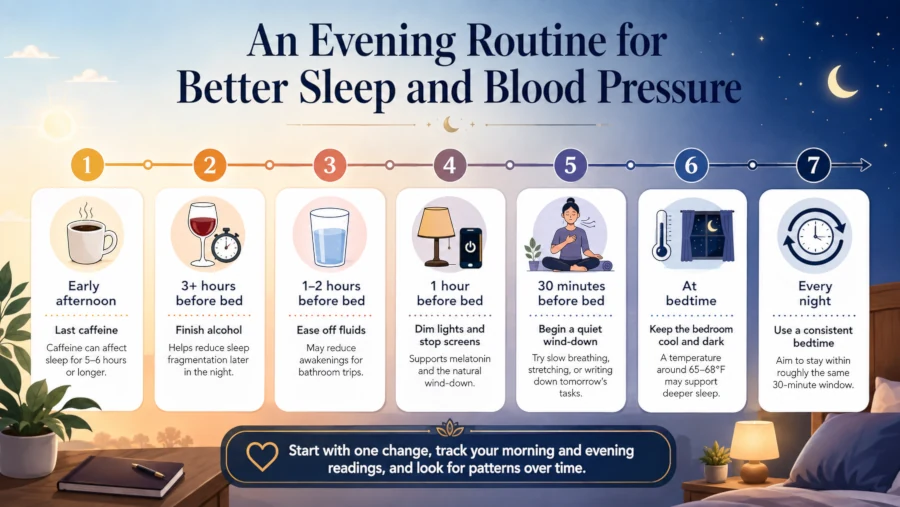
| Action | Timing | Why it helps |
| Last caffeine | Early afternoon | Effects can linger 5–6+ hours and shorten deep sleep |
| Last alcohol | 3+ hours before bed | Reduces the rebound sympathetic surge later in the night |
| Ease off evening fluids | Last 1–2 hours | Fewer awakenings to use the bathroom |
| Dim lights, off screens | Last hour | Supports melatonin and the overnight pressure dip |
| Cool the bedroom | Around 65–68°F | Helps deep sleep and the nocturnal dip |
| Wind-down routine | ~30 min before bed | Lowers the bedtime stress response |
| Consistent bedtime | Same ~30-min window | Stabilizes the circadian pattern |
A Two-Week Plan to See Your Own Pattern
Week 1: Get a baseline
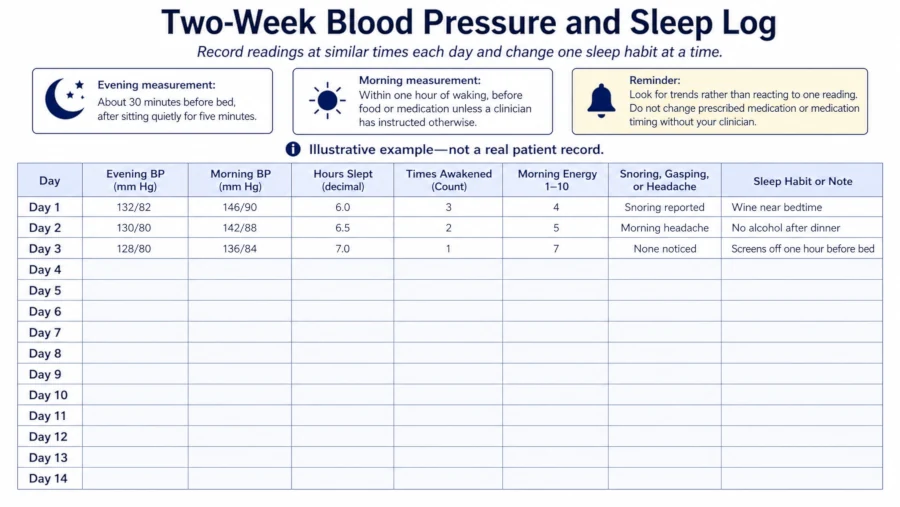
For seven days, check your blood pressure twice: in the evening (about 30 minutes before bed, after sitting quietly for five minutes) and in the morning (within an hour of waking, before food or medication). Record both. The gap between them is the number you’re watching. If you’re new to this, our guide to home blood pressure monitoring walks through accurate technique.
Alongside the numbers, jot down: estimated hours slept, how many times you woke, a 1–10 morning energy rating, and any snoring, gasping, or morning headaches a partner notices.
Week 2: Change one thing at a time
Pick a single change from the list above — alcohol timing is a common first choice — and hold everything else steady so you can actually see its effect. After a few days, layer in a second change. Keep recording.
An illustrative example (not a real patient): suppose your morning readings sit around 150/94 while your evenings are near 128/80, and you sleep poorly after wine most nights. You might stop alcohol on four nights the first week and watch the morning gap. If snoring and daytime tiredness are also in the picture, that’s a strong cue to ask for a sleep study rather than to keep adjusting habits on your own. Two drivers often compound — fixing one helps, fixing both can make the difference.
About Sleep Supplements: Melatonin and Magnesium
Set expectations first: supplements are a minor lever compared with treating apnea, cutting late alcohol, or protecting your sleep schedule. Fix those first.
Melatonin. The evidence here is promising but limited and specific. A meta-analysis found that controlled-release melatonin, taken as an add-on in people with confirmed nighttime hypertension, lowered nocturnal systolic pressure by around 6 mmHg — while ordinary fast-release melatonin showed no significant effect [Grossman meta-analysis, Vascular Health and Risk Management, 2011]. Worth knowing: the trials were small, several study authors were affiliated with a melatonin manufacturer, and this is not a substitute for fixing the underlying sleep problem. Melatonin can cause daytime grogginess, headache, or vivid dreams, and it may interact with blood thinners, blood-pressure and diabetes medications, sedatives, and some antidepressants. It isn’t recommended in pregnancy or breastfeeding without medical advice. Talk to a pharmacist or clinician before combining it with prescription drugs.
Magnesium. Some people use magnesium (for example, magnesium glycinate) to wind down. Evidence that it meaningfully lowers blood pressure is weak, so treat it as a possible sleep aid rather than a blood-pressure treatment. Higher doses commonly cause loose stools or diarrhea. It can interact with certain antibiotics and other medications, and — importantly — people with reduced kidney function can accumulate magnesium to dangerous levels, so anyone with kidney disease should not supplement without medical guidance. If you’re pregnant or breastfeeding, or take prescription medication, check with a clinician first.
Special Situations
If you’re over 60: your overnight dip may be naturally less pronounced, and that isn’t automatically dangerous. Focus on whether your daytime pressure is controlled and whether you feel rested. A complete absence of any nighttime fall still warrants a conversation with your clinician.
If you work shifts: aim for consistency within your own schedule — similar sleep and wake times on work days, blackout curtains for daytime sleep, and limits on caffeine and alcohol near your sleep window. Track blood pressure against your sleep-wake cycle, not the clock.
If your morning readings spike sharply: a large, consistent morning jump can prompt a discussion about medication timing. The evidence on morning versus bedtime dosing is genuinely mixed, and recent large trials have not shown a clear advantage to bedtime dosing — so this is a decision to make with your prescriber, never a change to try on your own. Our guide to the morning blood pressure surge explains the pattern in more detail.
If racing thoughts keep you awake: for ongoing insomnia, cognitive behavioral therapy for insomnia (CBT-I) is recommended as the first-line treatment for adults — ahead of sleep medications — by the American College of Physicians [American College of Physicians guideline, 2016], and it outperformed a first-generation behavioral approach and placebo in a randomized trial [Edinger, JAMA, 2001]. It’s more durable than sleeping pills and avoids their downsides.
When to See a Doctor — and When to Get Help Now
Track your numbers, but don’t wait on these:
- Your morning readings run consistently 20+ mmHg higher than your evening readings, or stay elevated despite medication and lifestyle changes.
- Loud snoring with gasping, choking, or witnessed pauses in your breathing during sleep.
- Waking with headaches or feeling unrefreshed despite 7–8 hours in bed.
- Daytime sleepiness that interferes with work or driving — don’t drive drowsy.
Treat as urgent: a blood pressure reading at or above 180/120 mmHg. If there are no symptoms, call your doctor or nurse line right away. If it comes with severe headache, chest pain, shortness of breath, vision changes, or trouble speaking, call 911 — this is a medical emergency. In the U.S., ongoing concerns are best handled through your primary care clinician, with urgent care or the ER for anything that can’t wait.
| Health Disclaimer: This article about sleep and blood pressure is for educational purposes only and is not medical advice. It cannot diagnose sleep apnea or any other condition — that requires objective testing and a qualified clinician. If you have high blood pressure, heart disease, kidney disease, are pregnant or breastfeeding, or take prescription medications, talk with a qualified clinician before changing treatment, diet, exercise, or supplements. Do not stop or adjust blood pressure medication — or its timing — without your prescriber. |
Frequently Asked Questions
Can poor sleep raise my blood pressure even if I’m otherwise healthy?
It’s associated with higher risk, yes. In adults, habitually short sleep was linked to roughly a 20% higher rate of high blood pressure [Wang, 2012]. Short sleep raises stress hormones and nervous-system activity, and experimental sleep restriction raises pressure — though for any one person, sleep is one of several contributing factors rather than the whole story.
How fast might my readings improve after I fix my sleep?
It depends on the cause. If late alcohol or caffeine was the issue, some people see a difference within a week or two. If sleep apnea is the driver, CPAP can shift pressure over several weeks, and consistent use matters — measurable benefit is often judged over about 12 weeks [CPAP resistant-hypertension meta-analysis, 2024].
Will a melatonin supplement lower my blood pressure?
Possibly a little, and only in a specific situation. Controlled-release melatonin modestly lowered nighttime pressure in people with confirmed nocturnal hypertension, while fast-release melatonin did not [Grossman, 2011]. It’s not a substitute for addressing the underlying sleep problem, and it can interact with several medications — check with a clinician first.
Should I check my blood pressure in the middle of the night?
Usually no. Evening and morning checks are enough to reveal the pattern for most people. Waking yourself to measure tends to raise anxiety and worsen sleep, which is counterproductive. Only do overnight checks if your clinician specifically asks you to.
I’m a shift worker — does any of this apply?
Yes, with a twist. Your circadian rhythm is already shifted, so consistency within your own schedule matters most: steady sleep and wake times on work days, blackout curtains, and limited caffeine and alcohol near sleep. Track your readings against your sleep-wake cycle rather than the clock.
Can stress alone keep my nighttime pressure up?
It can contribute. Ongoing stress keeps stress hormones and sympathetic activity elevated, which can blunt the normal overnight dip. For persistent insomnia tied to stress, CBT-I is the recommended first-line approach for adults [American College of Physicians, 2016], and it’s worth pursuing before sleep medications.
References
- American College of Cardiology. Prioritizing Health: Sleep and Cardiovascular Health. 2025. View source
- Salles GF, et al. Prognostic Effect of the Nocturnal Blood Pressure Fall in Hypertensive Patients (ABC-H Meta-Analysis). Hypertension. 2016;67(4):693–700. View source
- American Heart Association (newsroom). Abnormal blood pressure levels while sleeping increase risk of heart disease, stroke. 2020. View source
- Wang Q, et al. Short sleep duration is associated with hypertension risk among adults: a systematic review and meta-analysis. Hypertension Research. 2012;35(10):1012–1018. View source
- Makarem N, et al. Sleep Duration and Blood Pressure: Recent Advances and Future Directions. Current Hypertension Reports. 2023. View source
- Logan AG, et al. High prevalence of unrecognized sleep apnoea in drug-resistant hypertension. Journal of Hypertension. 2001;19(12):2271–2277. View source
- Chen Q, et al. Effect of CPAP on Blood Pressure in Patients With Resistant Hypertension and Obstructive Sleep Apnea: An Updated Meta-analysis. Current Hypertension Reports. 2024. View source
- Grossman E, Laudon M, Zisapel N. Effect of melatonin on nocturnal blood pressure: meta-analysis of randomized controlled trials. Vascular Health and Risk Management. 2011;7:577–584. View source
- Qaseem A, et al. Management of Chronic Insomnia Disorder in Adults: A Clinical Practice Guideline From the American College of Physicians. Annals of Internal Medicine. 2016;165(2):125–133. View source
- Edinger JD, et al. Cognitive behavioral therapy for treatment of chronic primary insomnia: a randomized controlled trial. JAMA. 2001;285(14):1856–1864. View source
- Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta-analysis. Journal of the American Heart Association. 2013;2(1):e004473. View source
- Vetter C, et al. Association Between Rotating Night Shift Work and Risk of Coronary Heart Disease Among Women. JAMA. 2016;315(16):1726–1734. View source