Cardiovascular and pulmonary disease is a broad term for conditions that affect the heart, the lungs, or both. Because these two systems are biologically linked — the heart pumps blood to the lungs for oxygen, and the lungs depend on steady blood flow to do their job — problems in one often ripple into the other. A lung condition can strain the heart; a weakening heart can leave the lungs congested [1, 4].
This guide explains what cardiovascular and pulmonary disease means, how the heart and lungs work together, and which conditions fall into each category.
It walks through the symptoms and risk factors to watch for, how doctors diagnose these illnesses, the treatment and rehabilitation options available, and the everyday steps that support long-term heart and lung health [2, 3].
The goal here is to inform, not alarm. Many of these conditions are manageable with early evaluation, coordinated care, and consistent follow-up — and the same healthy habits tend to protect both systems at once.
What Is Cardiovascular and Pulmonary Disease?
Cardiovascular disease (CVD) is an umbrella term for conditions that affect the heart or blood vessels, including coronary artery disease, heart failure, arrhythmias, stroke, and peripheral artery disease [1].
Pulmonary disease refers to disorders of the lungs and airways, such as chronic obstructive pulmonary disease (COPD), asthma, interstitial lung disease, pulmonary embolism, and lung infections [3].
The phrase “cardiovascular and pulmonary disease” is not a single diagnosis. It is a helpful way to describe how heart and lung diseases frequently occur together or influence one another. Some clinicians use the term cardiopulmonary disease when conditions involve both systems at once — for example, pulmonary hypertension that leads to right-sided heart failure [4].
Understanding this overlap matters because a patient with heart disease often has lung-related symptoms, and someone with chronic lung disease is at higher risk of developing heart problems [5].
How the Heart and Lungs Work Together
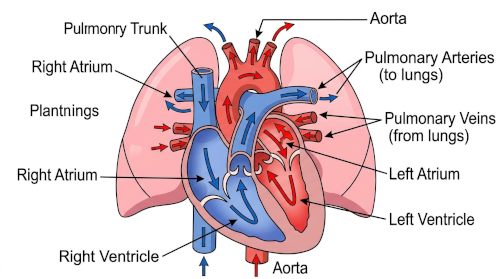
The heart and lungs share a continuous loop:
- Oxygen-poor blood from the body returns to the right side of the heart.
- The right ventricle pumps that blood into the lungs.
- In the lungs, tiny air sacs (alveoli) exchange carbon dioxide for oxygen.
- Oxygen-rich blood returns to the left side of the heart and is pumped out to the body [6].
This is called cardiopulmonary circulation. If the lungs cannot absorb oxygen well (for example, in severe COPD or pulmonary fibrosis), the right side of the heart must work harder, which can eventually cause a condition called cor pulmonale, or right-sided heart failure due to lung disease [4]. Conversely, when the left side of the heart weakens, fluid can back up into the lungs, causing pulmonary congestion and shortness of breath [1].
In short: heart problems can mimic or worsen lung problems, and lung problems can mimic or worsen heart problems. Sorting this out is a core task of diagnosis.
Common Cardiovascular Conditions
Coronary Artery Disease
CAD occurs when the arteries supplying the heart narrow, usually from plaque buildup (atherosclerosis). It can cause chest pain (angina) and, if an artery becomes blocked, a heart attack [1].
Heart Failure
Heart failure means the heart does not pump as efficiently as it should. It can affect the left side, right side, or both. Left-sided heart failure often causes breathlessness, especially when lying flat, because blood backs up into the lungs [1, 7].
Arrhythmias
Arrhythmias are abnormal heart rhythms, such as atrial fibrillation (AFib). AFib can raise stroke risk and is more common in people with chronic lung disease [8].
Pulmonary Hypertension
Pulmonary hypertension is high blood pressure in the arteries of the lungs. It can arise from lung disease, left-sided heart disease, blood clots, or other causes, and it puts strain on the right side of the heart [4, 9].
Common Pulmonary Conditions
Chronic Obstructive Pulmonary Disease
COPD is a progressive disease that causes airflow obstruction, often from long-term smoking or chronic exposure to lung irritants. Common symptoms include chronic cough, sputum production, and shortness of breath [3, 10].
Asthma

Asthma is a chronic airway disease that causes wheezing, coughing, chest tightness, and shortness of breath, often in response to triggers like allergens, exercise, or cold air [11].
Interstitial Lung Disease (ILD)
ILD is a group of conditions that cause scarring and inflammation of the lung tissue, leading to progressive shortness of breath and, in some cases, the need for supplemental oxygen [12].
Pulmonary Embolism
A pulmonary embolism occurs when a blood clot (usually from the legs) travels to the lungs. PE is a medical emergency that can cause sudden shortness of breath, chest pain, and low oxygen levels [13].
Pulmonary Hypertension
As noted earlier, pulmonary hypertension often stems from underlying lung disease and can lead to heart strain if not managed appropriately [4, 9].
Cardiovascular and pulmonary diseases share many risk factors, which is one reason they often occur together [1, 2, 14].
- Smoking and secondhand smoke – A leading cause of both CVD and COPD [14, 15].
- Air pollution – Long-term exposure raises risk of heart disease, stroke, and lung disease [16].
- High blood pressure (hypertension) – A major contributor to heart disease and stroke [1].
- Diabetes – Increases risk of CVD and may worsen respiratory outcomes [1].
- Obesity – Linked to heart disease, sleep apnea, and reduced lung function [17].
- Physical inactivity – Lowers cardiorespiratory fitness and raises cardiovascular risk [18].
- Sleep apnea – Associated with hypertension, AFib, heart failure, and pulmonary hypertension [19].
- Age and family history – Non-modifiable but important for risk assessment [1].
- Occupational exposures – Dust, fumes, silica, asbestos, and certain chemicals can damage the lungs and may affect cardiovascular health [20].
Symptoms to Watch For
Common Symptoms
- Shortness of breath during activity or at rest
- Chronic cough
- Wheezing
- Chest discomfort or tightness
- Fatigue, especially with exertion
- Swelling in the legs or ankles
- Reduced exercise tolerance
Symptoms That May Reflect Combined Heart–Lung Involvement
- Breathlessness when lying flat (orthopnea)
- Waking up at night gasping for air
- Persistent low oxygen levels
- Unexplained rapid or irregular heartbeat with breathlessness
- Bluish tint to lips or fingertips (cyanosis), especially with exertion [1, 3]
Emergency Warning Signs
Seek immediate medical care for:
- Sudden, severe chest pain or pressure
- Severe shortness of breath
- Bluish lips or face
- Fainting or near-fainting
- Sudden weakness on one side of the body, facial drooping, or difficulty speaking (possible stroke)
- Coughing up large amounts of blood [1, 13, 21]
These can be signs of a heart attack, pulmonary embolism, stroke, or severe heart or lung failure.
How Doctors Diagnose Cardiovascular and Pulmonary Disease
Because symptoms overlap, clinicians usually combine several tools [1, 3, 22]:
- History and physical exam – Includes listening to the heart and lungs, checking pulses, and assessing swelling.
- Blood pressure and pulse oximetry – Quick checks that can reveal important clues.
- Electrocardiogram (ECG) – Records the heart’s electrical activity.
- Echocardiogram – Ultrasound of the heart that shows how well it pumps and whether valves work properly.
- Chest X-ray – Screens for lung disease, enlarged heart, or fluid in the lungs.
- CT scan – Can show detailed lung anatomy or evaluate for pulmonary embolism.
- Pulmonary function tests (PFTs) – Measure how well the lungs move air and exchange gases; essential for diagnosing asthma, COPD, and ILD [3, 11].
- Blood tests – Including natriuretic peptides (BNP/NT-proBNP) for heart failure, D-dimer in suspected PE, and standard panels [7, 13].
- Stress testing – Evaluates how the heart responds to exertion.
- Right heart catheterization – A specialized procedure used when pulmonary hypertension is suspected. A small catheter is guided into the right side of the heart to measure pressures directly [9].

Diagnosis is usually a process, not a single test. Specialists in cardiology and pulmonology frequently collaborate.
Treatment Options
Treatment always depends on the specific diagnosis and must be individualized by a qualified clinician. Common categories include [1, 3, 10, 11]:
Lifestyle Interventions
- Quitting smoking (one of the most impactful steps) [15]
- Regular aerobic exercise as medically appropriate
- Heart-healthy eating patterns, such as Mediterranean or DASH-style diets [23]
- Weight management
- Limiting alcohol
Medications
Examples include (as prescribed):
- Blood pressure medications (ACE inhibitors, ARBs, beta-blockers, diuretics)
- Statins for cholesterol
- Antiplatelets or anticoagulants when indicated
- Bronchodilators and inhaled corticosteroids for asthma or COPD
- Medications specifically for pulmonary arterial hypertension [9]

Oxygen Therapy
Supplemental oxygen may be recommended for people with chronically low oxygen levels, particularly in advanced COPD or ILD [3, 10].
Rehabilitation
- Cardiac rehabilitation – Supervised exercise, education, and counseling after heart events or surgery [24].
- Pulmonary rehabilitation – Structured exercise and education for chronic lung disease; shown to improve breathlessness, exercise tolerance, and quality of life [25].
Procedures or Surgeries
Depending on the condition, these may include angioplasty with stenting, coronary bypass surgery, valve repair or replacement, catheter ablation for arrhythmias, or lung-related procedures such as bronchoscopy or, in select cases, lung volume reduction or transplant [1, 10].
Management of Underlying Risk Factors
Controlling blood pressure, cholesterol, diabetes, and sleep apnea is often central to treatment of both heart and lung disease [1, 19].
Prevention and Long-Term Management
Many cardiovascular and pulmonary diseases are at least partly preventable. Prevention strategies include [1, 3, 14, 15]:
- Not smoking, and avoiding secondhand smoke
- Vaccines when recommended, including influenza, pneumococcal, and COVID-19 vaccines for eligible individuals with chronic heart or lung conditions [26]
- Regular physical activity, tailored to medical status
- Cardiac and pulmonary rehabilitation when prescribed
- Blood pressure, cholesterol, and diabetes control
- Adherence to prescribed therapy, including inhalers and cardiovascular medications
- Follow-up care with primary care and specialists
- Reducing environmental exposures, including indoor and outdoor air pollution and occupational irritants [16, 20]
Multidisciplinary Care
People with overlapping heart and lung disease often do best with coordinated care involving primary care clinicians, cardiologists, pulmonologists, nurses, dietitians, physical therapists, and rehabilitation specialists [24, 25].
Prognosis and When to Seek Medical Attention
Outlook varies widely. Some conditions, like well-controlled asthma or stable coronary disease, can be managed for decades with a good quality of life. Others, like advanced heart failure or severe interstitial lung disease, are more serious. Key factors influencing prognosis include the exact diagnosis, severity, how early it is identified, the presence of other conditions, and how consistently treatment is followed [1, 3, 7].
When to contact your doctor (non-emergency):
- New or worsening cough, wheeze, or breathlessness
- Gradual decline in exercise tolerance
- New swelling in legs or ankles
- Unexplained fatigue
- Blood pressure or blood sugar that is consistently out of range
When to seek emergency care:
- Chest pain or pressure lasting more than a few minutes
- Severe or sudden shortness of breath
- Fainting
- Bluish lips or face
- Stroke symptoms (face drooping, arm weakness, speech difficulty)
- Coughing up significant amounts of blood [1, 13, 21]
When in doubt, it is safer to seek urgent evaluation than to wait.
Cardiovascular and pulmonary disease represents a broad but connected group of conditions affecting the heart and lungs. Because these organs work as partners, diseases in one system often ripple into the other — sometimes subtly, sometimes dramatically. Understanding the overlap helps patients recognize symptoms earlier, ask informed questions, and partner effectively with their healthcare team.
Most people benefit from the same foundational steps: avoiding tobacco, staying active within safe limits, eating a balanced diet, managing blood pressure and blood sugar, getting recommended vaccines, and keeping regular follow-up appointments. When symptoms do appear, early evaluation and coordinated care between cardiology, pulmonology, and primary care can make a meaningful difference.
Medical Disclaimer: This content is for educational purposes only. It is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of a qualified healthcare provider with any questions you may have about a medical condition. If you have symptoms of a medical emergency — such as severe chest pain, sudden shortness of breath, fainting, or stroke-like symptoms — call emergency services or go to the nearest emergency department immediately.
Cardiovascular vs Pulmonary Disease
| Category | Main Organs Affected | Common Examples | Typical Symptoms | Common Tests |
| Cardiovascular disease | Heart, arteries, veins | Coronary artery disease, heart failure, arrhythmias, stroke | Chest pain, breathlessness, fatigue, palpitations, leg swelling | ECG, echocardiogram, stress test, blood tests (e.g., BNP, troponin) |
| Pulmonary disease | Lungs, airways | COPD, asthma, interstitial lung disease, pulmonary embolism | Cough, wheezing, shortness of breath, sputum, low oxygen | Pulmonary function tests, chest X-ray, CT scan, pulse oximetry |
| Cardiopulmonary overlap | Heart + lungs | Pulmonary hypertension, cor pulmonale, heart failure with pulmonary congestion | Breathlessness, exercise intolerance, swelling, cyanosis | Echocardiogram, CT, PFTs, right heart catheterization |
| Risk Factor | Effect on Heart Health | Effect on Lung Health | Can It Be Modified? |
| Smoking | Accelerates atherosclerosis, raises heart attack and stroke risk | Leading cause of COPD and lung cancer | Yes |
| Air pollution | Increases heart disease and stroke risk | Worsens asthma, COPD, and lung function | Partly (reduce exposure) |
| High blood pressure | Strains the heart, increases stroke and heart failure risk | Can contribute to pulmonary hypertension when severe | Yes |
| Diabetes | Raises risk of CAD, heart failure, stroke | May worsen respiratory infections and outcomes | Often, with treatment |
| Obesity | Increases heart disease, hypertension, AFib risk | Associated with sleep apnea, reduced lung volumes | Often, with support |
| Physical inactivity | Lowers cardiovascular fitness | Reduces respiratory endurance | Yes |
| Sleep apnea | Linked to hypertension, AFib, heart failure | Contributes to low nighttime oxygen, pulmonary hypertension | Yes, with treatment |
| Age | Risk increases with age | Risk increases with age | No |
| Family history | Genetic predisposition to heart disease | Genetic predisposition to some lung diseases | No |
| Occupational exposures | May contribute to cardiovascular risk | Can cause occupational lung disease | Partly (with protection) |
Warning Signs and Recommended Action
| Symptom or Sign | Possible Concern | Recommended Action |
| Sudden severe chest pain or pressure | Heart attack, pulmonary embolism | Emergency Care (call 911) |
| Sudden severe shortness of breath | PE, heart failure flare, severe asthma attack | Emergency Care |
| Bluish lips or face | Low blood oxygen | Emergency Care |
| Fainting or near-fainting | Arrhythmia, low blood pressure, PE | Emergency Care |
| Stroke symptoms (face droop, arm weakness, speech trouble) | Stroke | Emergency Care |
| Coughing up significant blood | Serious lung or heart condition | Emergency Care |
| Gradual worsening breathlessness over weeks | Heart failure, COPD progression, ILD | Urgent Care or prompt doctor visit |
| New persistent cough | Asthma, COPD, infection, other causes | Routine or Urgent Care |
| New leg swelling | Heart failure, blood clot | Urgent Care |
| Mild exertional breathlessness that is new | Early heart or lung disease | Routine Care |
| Well-known, stable symptoms following a treatment plan | Known condition | Routine follow-up |
Frequently Asked Questions
What is the difference between cardiovascular and pulmonary disease?
Can lung disease affect the heart?
Yes. Chronic lung diseases like COPD or interstitial lung disease can raise the pressure in the lung arteries, straining the right side of the heart. Over time, this can lead to right-sided heart failure (cor pulmonale) [4].
Can heart disease cause shortness of breath?
Is COPD a cardiovascular or pulmonary disease?
What are the first warning signs?
Are these conditions preventable?
Many are at least partly preventable. Not smoking, staying active, eating well, controlling blood pressure and blood sugar, avoiding air pollution when possible, and getting recommended vaccines can all lower risk [14, 15, 16, 26].
When should I go to the ER?
Can you have both heart and lung disease at the same time?
Yes. Shared risk factors like smoking, aging, high blood pressure, and obesity mean many people have conditions affecting both systems. Coordinated care from a cardiologist and a pulmonologist is often helpful [5].
What tests will my doctor order?
References
- [ 1 ]. American Heart Association. Heart Disease and Stroke Statistics – Annual Update. https://www.heart.org/en/about-us/heart-and-stroke-association-statistics
- [ 2 ]. World Health Organization. Cardiovascular diseases (CVDs) – Fact sheet. https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds)
- [ 3 ]. National Heart, Lung, and Blood Institute (NHLBI). Lung Diseases. https://www.nhlbi.nih.gov/health-topics/all-topics/lung
- [ 4 ]. National Heart, Lung, and Blood Institute. Pulmonary Hypertension. https://www.nhlbi.nih.gov/health/pulmonary-hypertension
- [ 5 ]. Rabe KF, Hurst JR, Suissa S. Cardiovascular disease and COPD: dangerous liaisons? European Respiratory Review, 2018. https://err.ersjournals.com/
- [ 6 ]. National Heart, Lung, and Blood Institute. How the Lungs Work. https://www.nhlbi.nih.gov/health/lungs
- [ 7 ]. Heidenreich PA, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure. Circulation / JACC, 2022.
- [ 8 ]. January CT, et al. 2019 AHA/ACC/HRS Focused Update on the Management of Patients With Atrial Fibrillation. Circulation, 2019.
- [ 9 ]. Humbert M, et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. European Heart Journal / European Respiratory Journal, 2022.
- [ 10 ]. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of COPD. https://goldcopd.org
- [ 11 ]. Global Initiative for Asthma (GINA). Global Strategy for Asthma Management and Prevention. https://ginasthma.org
- [ 12 ]. American Thoracic Society / European Respiratory Society. Official clinical practice guidelines on idiopathic pulmonary fibrosis. https://www.thoracic.org
- [ 13 ]. Konstantinides SV, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism. European Heart Journal, 2020.
- [ 14 ]. Centers for Disease Control and Prevention. Heart Disease Risk Factors. https://www.cdc.gov/heartdisease/risk_factors.htm
- [ 15 ]. U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General, 2014.
- [ 16 ]. World Health Organization. Ambient (outdoor) air pollution. https://www.who.int/news-room/fact-sheets/detail/ambient-(outdoor)-air-quality-and-health
- [ 17 ]. Powell-Wiley TM, et al. Obesity and Cardiovascular Disease: AHA Scientific Statement. Circulation, 2021.
- [ 18 ]. Piercy KL, et al. The Physical Activity Guidelines for Americans. JAMA, 2018.
- [ 19 ] Yeghiazarians Y, et al. Obstructive Sleep Apnea and Cardiovascular Disease: AHA Scientific Statement. Circulation, 2021.
- [ 20 ]. American Thoracic Society. Occupational Lung Disease resources. https://www.thoracic.org
- [ 21. ] American Heart Association. Warning Signs of a Heart Attack. https://www.heart.org/en/health-topics/heart-attack/warning-signs-of-a-heart-attack
- [ 22 ]. Virani SS, et al. 2023 AHA/ACC Multisociety Guideline for the Management of Chronic Coronary Disease. Circulation, 2023.
- [ 23 ]. Arnett DK, et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease. Circulation, 2019.
- [ 24 ]. American Association of Cardiovascular and Pulmonary Rehabilitation (AACVPR). Cardiac Rehabilitation Guidelines. https://www.aacvpr.org
- [ 25 ]. Spruit MA, et al. ATS/ERS Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am J Respir Crit Care Med, 2013.
- [ 26 ]. Centers for Disease Control and Prevention. Vaccines for Adults with Chronic Heart or Lung Disease. https://www.cdc.gov/vaccines/adults/rec-vac/health-conditions.html