Most herbs for hair loss promise more than they deliver. A small number have been tested in real clinical trials, and the results are worth knowing before you spend money on a bottle of oil or a bag of capsules. The rest sit in the “traditional use” bucket — long folk history, weak human evidence. This guide separates the two honestly, walks through the main types of hair loss so you can match a strategy to a cause, and flags the safety issues most herb roundups skip.
Hair loss has many flavors. The American Academy of Dermatology notes that hereditary pattern hair loss — androgenetic alopecia — is the most common cause worldwide, and that other causes range from severe stress and pregnancy to thyroid disease, iron deficiency, certain medications, and tight hairstyles [AAD]. The herb that helps depends entirely on which type you have. Some herbs have small but real human data behind them. Many do not.
| The short version • Four herbs have human clinical trial data: rosemary oil, pumpkin seed oil, saw palmetto, and a thyme/rosemary/lavender/cedarwood blend. • None replaces minoxidil or finasteride for moderate-to-severe pattern hair loss — but they may help mild cases or sit alongside medical treatment. • Traditional herbs like nettle, castor oil, and watercress have very limited human evidence for hair growth, despite frequent claims to the contrary. • See a clinician first if shedding is sudden, patchy, painful, or paired with fatigue, irregular periods, or weight changes. |

Match the herb to the type of hair loss
Before any herb makes sense, the cause matters. Three patterns cover most cases, and each responds to different treatment.
Androgenetic alopecia (pattern hair loss)
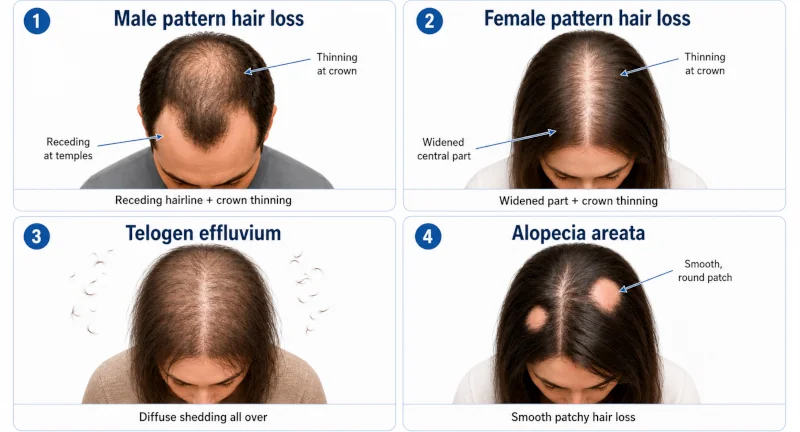
The most common form. In men, the hairline recedes and the crown thins; in women, the part widens and density drops on top, often years after a similar pattern would have started in men [Mayo Clinic, 2026]. Genetics and the hormone DHT (dihydrotestosterone) drive it. The FDA-approved standards are topical minoxidil and oral finasteride. Herbs that block DHT — saw palmetto, pumpkin seed oil — have human data here, though the effect is milder than prescription treatment. You can read more about how stress can interact with this pattern through general adaptogenic herbs.
Diffuse shedding that shows up two to three months after a trigger: high fever, COVID, surgery, childbirth, rapid weight loss, a new medication, or a sustained stressful event. The Mayo Clinic describes the mechanism as large numbers of follicles being pushed into a resting phase at the same time, with hair falling out a few months later when the next growth cycle begins [Mayo Clinic]. Hair usually regrows once the trigger passes. No herb will outperform fixing the underlying cause. If iron is the cause, foods rich in iron matter more than any scalp oil.
Alopecia areata (autoimmune patchy loss)
Round, smooth patches of bare scalp from the immune system attacking hair follicles. The American Family Physician review puts prevalence at roughly 0.1–0.2% of the population at any one time [AAFP, 2017]. Conventional treatment includes corticosteroid injections, topical immunotherapy, and newer JAK inhibitors. A 1998 randomized trial of an essential-oil blend (covered below) is one of the better natural-medicine signals in this area. Severe or rapidly progressing cases benefit from immunomodulation under a dermatologist.
Other causes that need their own fix
Iron deficiency anemia, low ferritin, thyroid disease (hypo- or hyperthyroid), protein malnutrition, traction from tight braids or ponytails, excessive vitamin A intake, scalp infections, and chemotherapy each have their own root cause. A scalp oil will not undo low iron or an untreated thyroid problem. Get the lab work done first.
Herbs for hair loss with the strongest human evidence
Four herbal approaches have been tested in proper randomized trials in people — not just lab studies on isolated cells or rodents. None is a cure, all have limitations, but the data is meaningful.
1. Rosemary oil (Rosmarinus officinalis)
This is probably the most-cited natural option for pattern hair loss. A 2015 randomized comparative trial published in Skinmed enrolled 100 adults with androgenetic alopecia. Half applied topical rosemary oil daily; half used 2% minoxidil. After six months, both groups showed a significant increase in hair count, with no significant difference between them, and scalp itching was less common in the rosemary group [Panahi et al., 2015]. One trial in 100 people is not the same as a settled treatment, and the comparison was to the lower-strength minoxidil (5% is more potent), but the result is genuinely interesting.
How it is used in research: diluted to roughly 1–2% in a carrier oil (about 5 drops of rosemary essential oil per tablespoon of jojoba, coconut, or grapeseed), massaged into the scalp once daily, with results assessed at six months. Never apply undiluted essential oil to skin — it can burn.

2. Pumpkin seed oil (Cucurbita pepo) — oral
A 2014 randomized, double-blind, placebo-controlled trial in 76 men with mild-to-moderate androgenetic alopecia gave 400 mg of oral pumpkin seed oil per day for 24 weeks. The active group had roughly a 40% increase in hair count versus about 10% in placebo, and self-rated improvement scores were significantly higher [Cho et al., 2014]. Pumpkin seed oil is believed to inhibit 5-alpha reductase, the enzyme that converts testosterone to DHT.
Caveats: small trial, men only, just 24 weeks. Some pumpkin seed oil capsules on the market contain only 100–200 mg per softgel, so check the label — the Cho trial used 400 mg/day. Topical pumpkin seed oil has separately been tested against minoxidil 5% foam in women with female pattern hair loss with some benefit, but the oral data remains the stronger signal.
3. Saw palmetto (Serenoa repens)
Used for prostate symptoms for decades and now studied for hair loss because it blocks DHT. A 2020 systematic review in Skin Appendage Disorders pooled five randomized clinical trials and two prospective cohort studies on saw palmetto for androgenetic alopecia and telogen effluvium. Across studies, about 60% of patients reported improved hair quality, 27% showed measurable hair-count increases, and 83% had increased hair density on investigator assessment [Evron et al., 2020]. Doses were 100–320 mg/day, oral or topical.
How it compares to prescription treatment: a 24-month head-to-head study put saw palmetto 320 mg/day against finasteride 1 mg/day. Finasteride was clearly more effective for hair density, but saw palmetto did beat baseline. Realistic positioning: a mild option for early pattern hair loss, not a replacement for prescription treatment, and worth discussing with a clinician before starting.
4. Essential-oil blend for alopecia areata
A 1998 randomized, double-blind, controlled trial at Aberdeen Royal Infirmary tested daily scalp massage with a blend of thyme, rosemary, lavender, and cedarwood essential oils (in jojoba and grapeseed carrier oils) on 86 patients with alopecia areata. After seven months, 44% (19 of 43) of the treatment group improved on blinded photographic assessment, compared with 15% (6 of 41) in the carrier-oil-only group [Hay et al., 1998]. Published in Archives of Dermatology, the trial has not been definitively replicated, but it remains one of the cleanest natural-medicine trials on alopecia areata.
Specific oil amounts from the protocol: thyme (88 mg), lavender (108 mg), rosemary (114 mg), cedarwood (94 mg) per application, mixed in 23 mL of carrier oil, massaged into bare patches for two minutes, covered with a warm towel for an hour, daily. Not a quick fix, and best supervised by a clinician who is treating the alopecia areata.
Traditional herbs for hair loss — what the evidence actually says
The herbs most commonly listed in folk-medicine roundups have far weaker science behind them than the four above. They are not necessarily useless — some have mild conditioning, anti-inflammatory, or astringent properties that may help scalp health — but the claims that they “regrow,” “regenerate,” or “stop” hair loss are not supported by human clinical trials. Here is an honest summary.
| Herb | Traditional use | Human clinical evidence for hair loss | Realistic positioning |
| Stinging nettle (Urtica dioica) | Scalp rinses and oral infusions for shedding; folk DHT blocker. | In-vitro and animal data suggest mild 5α-reductase inhibition. No good randomized human trials specifically for hair loss. | May support scalp health as a rinse; not a proven regrowth treatment. |
| Castor oil (Ricinus communis) | Scalp and brow oil; thought to thicken hair. | No published human clinical trials showing hair regrowth. Anecdotal popularity is high; case reports of acute hair felting (irreversible matting) exist. | Conditions hair; use sparingly and do not leave on overnight in thick layers. |
| Watercress (Nasturtium officinale) | Topical poultice and juice for scalp; eaten for iron and vitamin C. | No human trials for hair loss. Nutritional value (iron, vitamin C, vitamin K) is real. | Eat it for nutrition that supports hair generally; do not expect topical regrowth. |
| Maidenhair fern (Adiantum capillus-veneris, “Venus’ hair”) | Decoctions used in traditional European herbalism for hair strengthening. | No published human trials for hair growth or loss. | Traditional use only; safety in long-term scalp application is not well characterized. |
| Avocado (Persea americana) | Avocado oil and pulp used as a hair mask for shine and softness. | No randomized trials for hair regrowth. Cosmetic/conditioning benefit is plausible from monounsaturated fats and vitamin E. | Useful as a moisturizing mask; not a regrowth treatment. |
| Cinchona (Cinchona officinalis) | Bark decoction historically applied as a scalp “invigorator.” | No modern human trials for hair loss. Quinine, its main alkaloid, is a malaria drug; topical use can cause contact dermatitis. | Not recommended without a clinician’s guidance; risk-to-benefit unclear. |
| Nasturtium (Tropaeolum majus) | Topical “stimulating” lotion; included in some European hair tonics. | Some patented extracts have small studies showing changes to hair growth markers; high-quality independent trials are scarce. | Of interest but not yet validated; do a patch test — isothiocyanates can irritate skin. |
If you want to read the deeper traditional-use profiles for these plants, the site has full write-ups on stinging nettle, watercress, maidenhair fern (Venus’ hair), the castor bean plant, avocado, the cinchona tree, and nasturtium.
What herbs can’t do
Worth being plain about this. No herb has been shown to:
- Regrow hair on scar tissue or a smooth, shiny patch (scarring alopecia is generally permanent without a transplant).
- Reverse advanced bald areas where follicles are already gone.
- Replace fixing an underlying cause — iron deficiency, thyroid disease, protein deficiency, or a medication that’s triggering shedding.
- Match the effect size of finasteride for moderate-to-severe pattern hair loss, or topical steroids/JAK inhibitors for active alopecia areata.
If a product page promises full regrowth in a few weeks, the math is wrong — hair grows about half an inch per month, and clinical trials of the herbs above ran six months or longer before showing significant change.
Realistic expectations and a sensible timeline
Hair grows roughly 0.5 inches (1.25 cm) per month. The randomized trials cited here ran between 24 weeks (Cho 2014, pumpkin seed oil) and 7 months (Hay 1998, essential-oil blend), and most reported visible improvement around the four-to-six-month mark.
A few practical notes if you decide to try a herb that has clinical data:
- Give it at least three to six months before judging it. Earlier than that, you’re looking at noise in the hair cycle.
- Take baseline photos in the same lighting, same hairstyle, same time of day. Memory is unreliable; photographs are not.
- Change one variable at a time. Adding rosemary oil, pumpkin seed oil, biotin, and a new shampoo at once means you won’t know which (if any) helped.
- Stop if you notice scalp irritation, rash, or worsening shedding within the first few weeks.

Safety, side effects, and who should avoid herbs for hair loss
Herbal does not mean harmless. The data is best for short-term use of the herbs above, and there are real interactions and contraindications.
| Herb / product | Common side effects and interactions | Who should avoid |
| Rosemary oil (topical) | Contact dermatitis, scalp irritation, allergic reaction. Burns skin if used undiluted. | Pregnant or breastfeeding women, children, anyone with a known fragrance allergy. |
| Pumpkin seed oil (oral) | Generally well tolerated. Doses above 400 mg can cause mild GI upset. Theoretical blood-pressure-lowering effect. | Caution with antihypertensive medication; talk to a clinician if pregnant or on hormone-sensitive therapies. |
| Saw palmetto (oral or topical) | Nausea, dizziness, headache, mild GI upset. Anti-androgenic activity may interact with hormone therapy and anticoagulants. | Pregnant or breastfeeding women, anyone on warfarin, hormone therapy, oral contraceptives, or being worked up for prostate disease. |
| Essential-oil blend (thyme/rosemary/lavender/cedarwood) | Skin sensitization, contact dermatitis. Lavender has weak estrogenic activity in some reports. | Pregnant women, prepubertal children, anyone with a history of essential-oil reactions. |
| Castor oil | Rare reports of acute hair felting (sudden, irreversible matting) when used heavily on long hair. Scalp irritation possible. | Anyone with long or fine hair prone to tangling; use sparingly. |
| Nettle, watercress, maidenhair fern, cinchona, nasturtium | Contact dermatitis, irritation, allergy. Cinchona bark can cause quinine-type reactions in sensitive people. | Patch test first; avoid prolonged scalp use without medical guidance. |
Two interaction points worth flagging plainly. First, saw palmetto and pumpkin seed oil both touch the androgen pathway, which means anyone taking finasteride, dutasteride, or hormone therapy should clear them with a clinician before stacking. Second, essential oils — even diluted — can sensitize over time; if scalp itching or rash appears, stop.
When to see a doctor instead of reaching for an herb
These signs are reasons to see a primary care clinician or dermatologist rather than start an herbal regimen:
- Patchy, sudden hair loss in defined round spots, or eyebrow/eyelash loss — possible alopecia areata.
- Burning, pain, scaling, redness, or pus on the scalp — possible scarring alopecia or infection, both of which can become permanent without prompt treatment.
- Hair coming out in clumps after a stressful event, illness, surgery, or rapid weight change — likely telogen effluvium; a clinician can rule out reversible causes.
- Shedding paired with fatigue, cold intolerance, irregular periods, unexplained weight change, or new acne and facial hair — could be thyroid disease, anemia, or polycystic ovary syndrome.
- Visible scarring, smooth shiny bald patches, or a receding hairline at the temples in a child or young adolescent.
- Hair loss after starting a new prescription medication — ask the prescriber before stopping; many cases resolve when the dose is adjusted.

| Health Disclaimer This article is for general education only. It is not medical advice and should not be used to self-diagnose or self-treat. Hair loss can be a sign of an underlying condition — thyroid disease, iron deficiency, alopecia areata, polycystic ovary syndrome, scalp infection, or scarring alopecia, among others — and the right next step depends on the cause. Talk to a primary care clinician or dermatologist before starting any herb or supplement for hair loss, especially if you are pregnant or breastfeeding, taking prescription medication (including finasteride, dutasteride, hormone therapy, anticoagulants, or antihypertensives), being treated for a hormone-sensitive condition, or giving the product to a child. Stop any topical product immediately if you develop scalp pain, blistering, rash, or sudden worsening of shedding, and seek medical care. |
Frequently asked questions
Does rosemary oil really work as well as minoxidil?
In a 100-person trial, topical rosemary oil produced a hair-count increase similar to 2% minoxidil at six months, with less scalp itching [Panahi et al., 2015]. That is one trial, against the lower-strength minoxidil. It does not prove rosemary oil equals 5% minoxidil, the more potent FDA-approved formulation. Reasonable read: a credible mild option, not a proven replacement.
How long before I see results?
The clinical trials cited here ran six to seven months before they showed meaningful improvement. Give any herbal protocol at least three months before judging, and longer (six months) if you can be patient. Hair grows about half an inch per month, so visible change takes time.
Can I combine herbs with minoxidil or finasteride?
Possibly, but talk to your clinician first. Saw palmetto and pumpkin seed oil both touch the androgen pathway and can compound with finasteride or dutasteride. Topical rosemary oil is unlikely to interact with topical minoxidil, but combining two scalp products increases the chance of irritation. Layering more is not always better.
Are these herbs safe during pregnancy or breastfeeding?
No. Saw palmetto, pumpkin seed oil supplements, rosemary essential oil, and the thyme/rosemary/lavender/cedarwood blend are all on the avoid-in-pregnancy list for most herbal references. Postpartum shedding (a form of telogen effluvium) typically resolves on its own within 6–12 months; a clinician can confirm and rule out other causes.
What’s the single best herb for thinning hair?
There isn’t one. The herb with the most direct evidence for hereditary pattern hair loss is probably rosemary oil topically; for diffuse DHT-driven thinning, pumpkin seed oil orally or saw palmetto. For alopecia areata, the 1998 Hay essential-oil protocol has the cleanest data. None of these is a cure, and all of them work better when the underlying cause is identified.
References
- American Academy of Dermatology. Hair loss: who gets and causes. Accessed 2026. → View source
- Mayo Clinic. Hair loss — symptoms and causes. 2026. → View source
- Mayo Clinic. Stress and hair loss: are they related? 2023. → View source
- Phillips TG, Slomiany WP, Allison R. Hair loss: common causes and treatment. American Family Physician. 2017;96(6):371–378. → View source
- Panahi Y, Taghizadeh M, Marzony ET, Sahebkar A. Rosemary oil vs minoxidil 2% for the treatment of androgenetic alopecia: a randomized comparative trial. Skinmed. 2015;13(1):15–21. → View source
- Cho YH, Lee SY, Jeong DW, et al. Effect of pumpkin seed oil on hair growth in men with androgenetic alopecia: a randomized, double-blind, placebo-controlled trial. Evidence-Based Complementary and Alternative Medicine. 2014;2014:549721. doi:10.1155/2014/549721. → View source
- Evron E, Juhasz M, Babadjouni A, Mesinkovska NA. Natural hair supplement: friend or foe? Saw palmetto, a systematic review in alopecia. Skin Appendage Disorders. 2020;6(6):329–337. doi:10.1159/000509905. → View source
- Hay IC, Jamieson M, Ormerod AD. Randomized trial of aromatherapy. Successful treatment for alopecia areata. Archives of Dermatology. 1998;134(11):1349–1352. → View source
- Almohanna HM, Ahmed AA, Tsatalis JP, Tosti A. The role of vitamins and minerals in hair loss: a review. Dermatology and Therapy. 2019;9(1):51–70. → View source
- Allam AT, El-Shiekh RA, El-Dessouki AM, et al. Pathophysiology, conventional treatments, and evidence-based herbal remedies of hair loss with a systematic review of controlled clinical trials. Naunyn-Schmiedeberg’s Archives of Pharmacology. 2025. → View source