Hiatal hernia and gastric sleeve surgery come up together far more than most people expect. The reason is plain: the same years of carrying extra weight that lead someone toward weight-loss surgery also make a hiatal hernia more likely. So surgeons often find one while planning or performing the other.
The short version is that these are two different problems involving the same neighborhood — the spot where your stomach meets your esophagus. They connect in three practical ways. A surgeon often discovers a hiatal hernia during a sleeve operation and repairs it on the spot. A hernia left alone can worsen acid reflux afterward. And in some people, a hernia turns up months or years after the sleeve.
What a hiatal hernia actually is
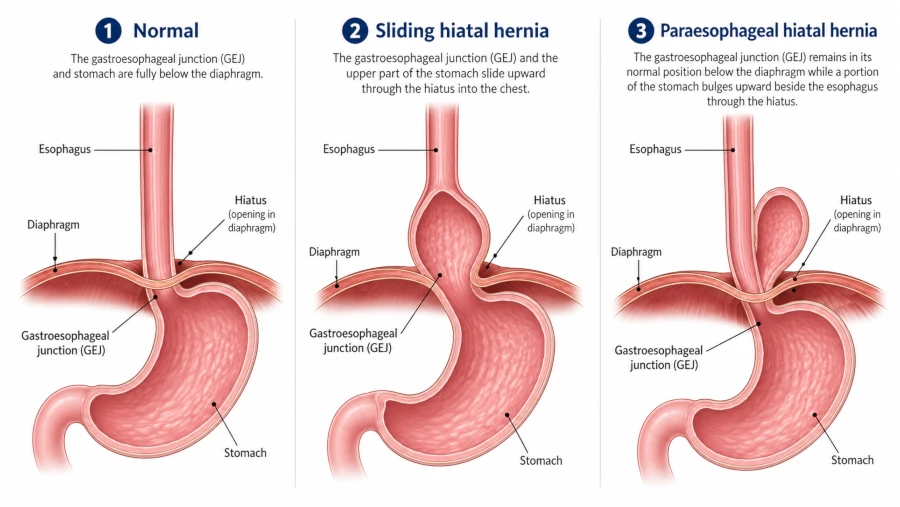
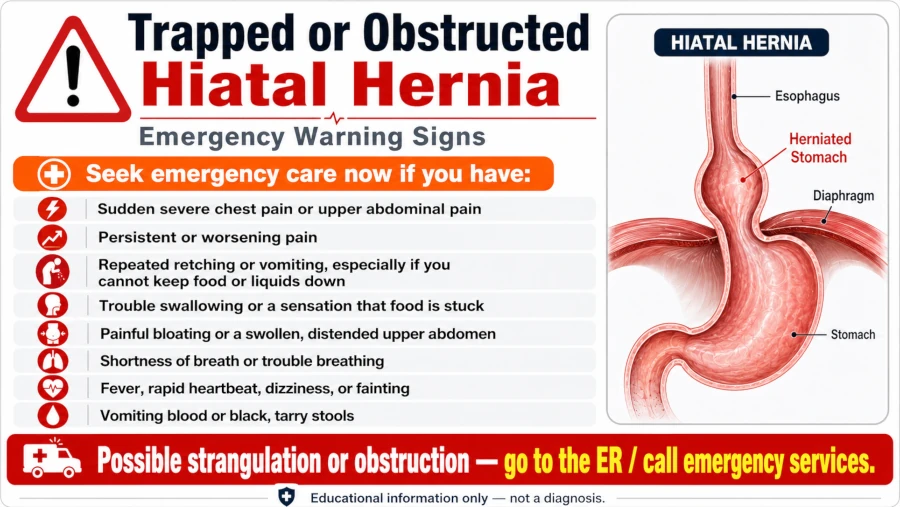
Your diaphragm is the dome of muscle that separates your chest from your belly and powers your breathing. It has a small opening, the hiatus, where the esophagus passes through to reach the stomach. A hiatal hernia happens when the upper part of the stomach pushes up through that opening into the chest. [Mayo Clinic, 2024]
Most hiatal hernias fall into one category. Roughly 95% are sliding hernias, where the junction of the stomach and esophagus slides up and back down through the hiatus. [StatPearls, 2026] The rest are paraesophageal hernias, where part of the stomach squeezes up alongside the esophagus and stays there. Those are less common but more likely to cause mechanical trouble.
Plenty of people have a hiatal hernia and never know it. When symptoms do appear, they usually trace back to acid reflux: heartburn, a sour taste, food or liquid coming back up, chest discomfort, and trouble swallowing. [Cleveland Clinic, 2025]
What gastric sleeve surgery does
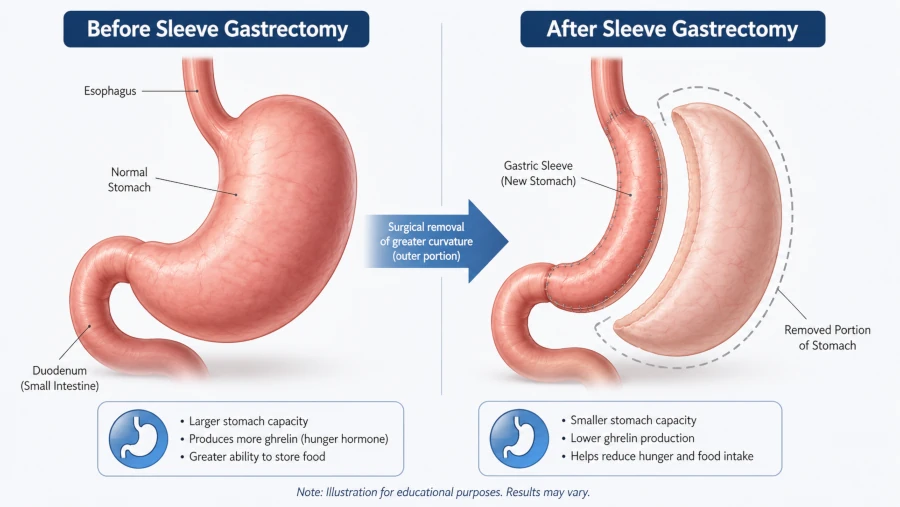
Gastric sleeve surgery, or sleeve gastrectomy, removes about 80% of the stomach and leaves a narrow tube roughly the size and shape of a banana. [Cleveland Clinic, 2025] It works two ways. The smaller stomach holds far less food, so you feel full sooner. And because the removed portion makes much of the body’s ghrelin — a hormone that drives appetite — hunger usually drops too. [Mayo Clinic, 2024]
It is now the most common weight-loss operation in the United States, making up more than 65% of bariatric procedures, with over 750,000 performed between 2018 and 2022. [Chen-Goodspeed et al., 2025] Most people lose a large share of their excess weight over the first one to two years, and conditions like type 2 diabetes and high blood pressure often improve.
Two different things, side by side
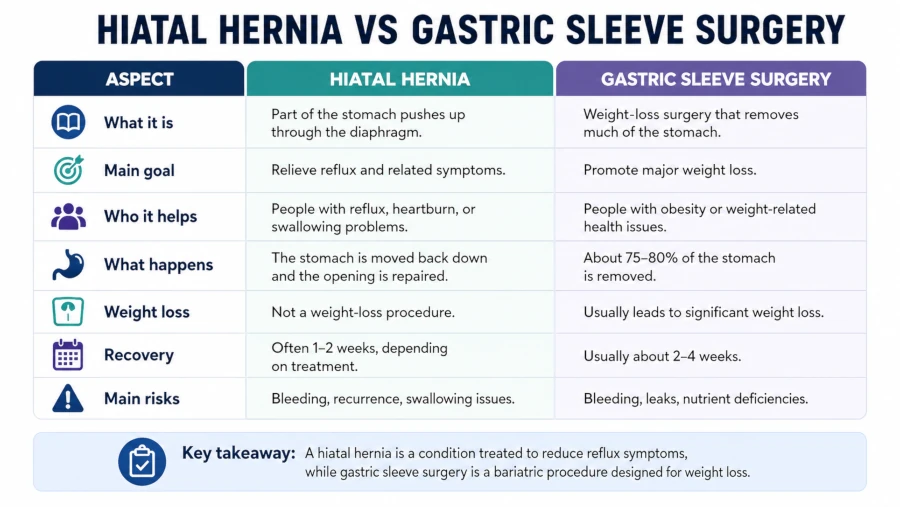
| Hiatal hernia | Gastric sleeve surgery | |
| What it is | A condition — the upper stomach pushes through the diaphragm | A procedure — about 80% of the stomach is removed |
| Main concern | Acid reflux (GERD) | Weight loss and metabolic health |
| Problem vs. fix | Something the body develops | Something a surgeon performs |
| The overlap | Common in people with obesity | Often reveals or worsens a hernia and reflux |
Why the two show up together
Excess weight raises pressure inside the abdomen. That steady upward push strains the thin membrane anchoring the stomach below the diaphragm, and over time it can let the junction creep upward and a hernia form. [StatPearls, 2026] The same pressure also worsens reflux. That is why hiatal hernias are common among people heavy enough to consider bariatric surgery, and why a pre-operative workup sometimes turns up one the person never suspected.
Reflux is the thread tying these conditions together. A sliding hiatal hernia weakens the body’s natural anti-reflux barrier, and somewhere between half and the large majority of people with diagnosed GERD also have one. [StatPearls, 2026]
The reflux question after a sleeve
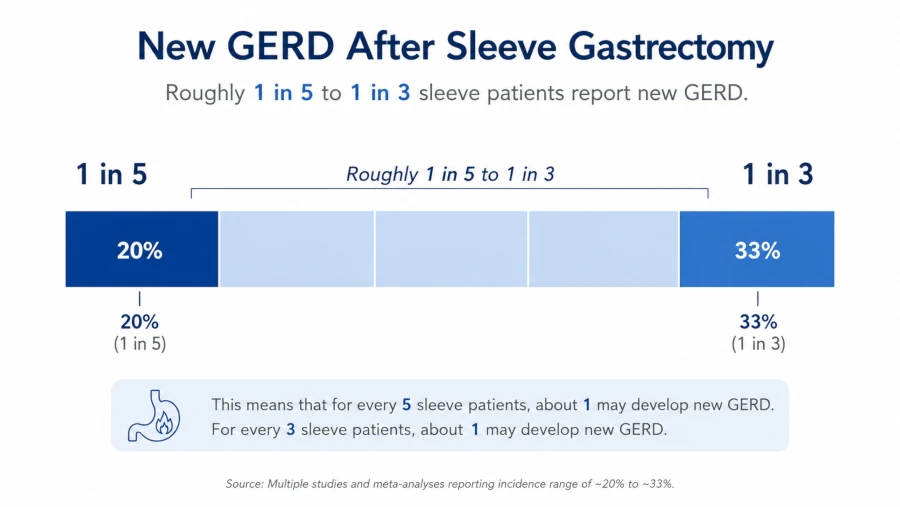
Here is the part that surprises people: a sleeve gastrectomy can make reflux worse, not better. Reshaping the stomach into a high-pressure tube, and trimming part of the natural valve mechanism, leaves some patients with new or worsened reflux. Estimates vary, but roughly 1 in 5 to 1 in 3 patients report new reflux after a sleeve, and studies using objective testing sometimes put it higher. [Almutairi et al., 2022] An unrecognized or untreated hiatal hernia is one of the things that makes this more likely.
Repairing the hernia during surgery
When a surgeon finds a hiatal hernia while performing a sleeve, current practice is to repair it in the same operation — usually by pulling the stomach back into the abdomen and tightening the diaphragm opening with sutures. [Chen et al., 2021] Whether that actually prevents reflux down the line is still debated, and the honest answer is that the evidence is mixed.
A 2021 systematic review and meta-analysis pooled studies on the combined sleeve-plus-hernia-repair. Reflux went into remission in about 68% of those patients, while roughly 12% developed new reflux and about 11% saw the hernia return. The combined approach beat the sleeve alone for reflux remission, with close to three times the odds. [Chen et al., 2021] The authors added an important caveat: most of those results lean on patients reporting symptoms rather than objective measurements, so they called for stronger studies before treating the benefit as settled. Some randomized data on small hernias have shown no clear difference at one year.
For a closer look at when a hernia needs fixing and whether its size matters, see our guide to hiatal hernia treatment options.
When a sleeve may not be the best fit
For some people, a large hiatal hernia or significant pre-existing reflux shifts the recommendation away from a sleeve. A Roux-en-Y gastric bypass tends to control reflux better, because it routes acid away from the esophagus, so surgeons sometimes suggest it — paired with hernia repair — when reflux is already a major problem. [Mayo Clinic, 2024] This is a conversation worth having before you choose a procedure, not after.
Hernias that appear after a sleeve
A hiatal hernia can also develop or come back after a sleeve, sometimes years later. Most cases show up as creeping reflux and are managed without drama. Rarely, the upper stomach becomes trapped, twisted, or obstructed — a situation that needs urgent attention rather than a wait-and-see approach. Case reports describe sleeve patients developing hernia-related obstruction as long as three years after surgery. [Chen-Goodspeed et al., 2025]
How doctors check
A few tests sort this out. An upper endoscopy lets the doctor look directly at the junction of the stomach and esophagus. A barium swallow X-ray shows the anatomy in motion. And esophageal manometry, which measures the pressure and muscle coordination of the esophagus, helps clarify how well the anti-reflux mechanism is working — useful before a second operation. [Mayo Clinic, 2024]
Managing symptoms day to day
If you have reflux from a hiatal hernia, whether or not surgery is on the table, some habits genuinely help: smaller meals, staying upright for a couple of hours after eating, raising the head of the bed, and limiting late-night food. What you eat matters too; our list of foods to eat with a hiatal hernia covers gentler choices that tend to trigger fewer symptoms. After a sleeve, rebuilding a steady, attentive relationship with food supports both recovery and reflux — the ideas behind intuitive eating can help here, working alongside your surgical team’s plan rather than replacing it. None of this closes the opening in the diaphragm, but it can take the edge off symptoms.
Realistic expectations
Surgery is a tool, not a guarantee. A sleeve can produce major, lasting weight loss and improve serious health conditions, but it can also introduce or worsen reflux, and a repaired hernia can recur. Most people do well. Some need follow-up procedures, including conversion to a bypass when reflux turns severe and does not respond to medication. Going in with clear expectations — and a surgeon who screens for hernias carefully — puts you in the strongest position.
Before you decide
- If you already have frequent heartburn or a known hiatal hernia, raise it early. It may change which procedure fits you.
- Ask your surgeon how often they screen for and repair hiatal hernias during a sleeve, and how they handle reflux that shows up later.
- Expect a thorough pre-operative evaluation. Finding a silent hernia before surgery beats discovering it after symptoms start.
Safety: when to get help
Routine reflux is annoying but rarely an emergency. A few symptoms are different and should not wait.
| Get urgent care if you have | Why it matters |
| Sudden, severe chest or upper-belly pain | Could signal a trapped (incarcerated) or strangulated hernia |
| Vomiting or retching with little or nothing coming up | May mean the stomach is twisted or obstructed |
| Inability to swallow or keep food and liquid down | Possible obstruction at the stomach-esophagus junction |
| Shortness of breath alongside the above | The hernia or trapped stomach may be pressing on the chest |
Chest pain can also be a heart problem. If you are not sure what you are dealing with, treat it as an emergency and get evaluated. [Cleveland Clinic, 2025] For ongoing but non-urgent reflux — heartburn most days, a sour taste, mild trouble swallowing — book a visit with your doctor or surgical team rather than pushing through it.
| HEALTH DISCLAIMER This article is for general education and information only. It is not medical advice and is not a substitute for diagnosis or treatment from a qualified clinician. Decisions about weight-loss surgery, hiatal hernia repair, or reflux treatment depend on your individual health, and only a licensed healthcare professional who knows your history can give personal guidance. If you are pregnant, breastfeeding, or have an existing medical condition, talk to your doctor before changing medications, diet, or treatment. If you have severe chest pain, cannot swallow, or cannot keep food or liquid down, seek emergency care. |
Frequently asked questions
Can you have gastric sleeve surgery if you already have a hiatal hernia?
Usually yes. Surgeons often repair the hernia during the same operation. A large hernia or significant pre-existing reflux, though, can make a gastric bypass the better choice, so it is worth discussing your options beforehand. [Mayo Clinic, 2024]
Does fixing a hiatal hernia during a sleeve prevent acid reflux?
It may reduce it. In a 2021 meta-analysis, combined repair outperformed the sleeve alone, with reflux remission near 68%. But those results rely mostly on symptom reports, the benefit is not guaranteed, and a small share of patients still develop reflux. [Chen et al., 2021]
Can a hiatal hernia come back after gastric sleeve surgery?
Yes. Recurrence was reported in roughly 1 in 10 combined-repair patients, and new hernias can appear later, sometimes years after surgery. [Chen et al., 2021]
Why does a gastric sleeve sometimes cause reflux?
The narrow, higher-pressure stomach tube and changes to the valve where the esophagus meets the stomach can both promote reflux. Roughly 1 in 5 to 1 in 3 sleeve patients report new reflux. [Almutairi et al., 2022]
Is gastric bypass better than a sleeve if I have reflux?
For significant pre-existing reflux or a large hernia, a Roux-en-Y bypass often controls reflux better and may be recommended over a sleeve. Your surgeon can weigh this against your other goals and health factors. [Mayo Clinic, 2024]
References
- Mayo Clinic. Hiatal hernia — Symptoms and causes. 2024. → View source
- Mayo Clinic. Sleeve gastrectomy — About. 2024. → View source
- Mayo Clinic. Esophageal manometry. 2024. → View source
- Mayo Clinic. Weight-loss surgery: Is it an option for you? 2024. → View source
- Cleveland Clinic. Hiatal hernia. 2025. → View source
- Cleveland Clinic. Gastric sleeve surgery (sleeve gastrectomy). 2025. → View source
- Smith MS, et al. Hiatal Hernia. StatPearls, NCBI Bookshelf. 2026. → View source
- Chen W, Feng J, Wang C, et al. Effect of Concomitant Laparoscopic Sleeve Gastrectomy and Hiatal Hernia Repair on GERD in Patients with Obesity: a Systematic Review and Meta-analysis. Obes Surg. 2021;31(9):3905–3918. → View source
- Almutairi BF, Aldulami AB, Yamani NM. GERD and Hiatal Hernia After Laparoscopic Sleeve Gastrectomy: A Retrospective Cohort Study. Cureus. 2022;14(3):e23024. → View source
- Chen-Goodspeed A, Kim A, Schmiederer I, Ricci-Gorbea J. Gastric Fundus Obstruction From Hiatal Hernia After Sleeve Gastrectomy: A Case Report. Cureus. 2025. → View source