
A series of medical techniques have been designed to help overcome fertility problems. The main methods are artificial insemination, in vitro fertilization (IVF), and surrogate motherhood.
These techniques deserve to be examined from a medical perspective and a social, ethical, and legal point of view. However, we cannot possibly address all these issues. We can only give general information in the hope of their own opinion on the matter or can contrast their view with others if they already have an idea.
We also hope to give enough basic information so that one with a particular interest in the subject can study it more deeply elsewhere.
Artificial Insemination
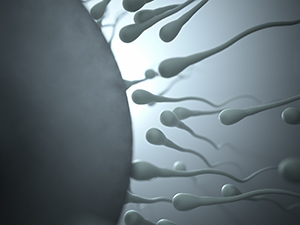
Artificial insemination consists of introducing male semen into the vagina using technological methods which have been developed to assist in producing a pregnancy. This semen, which often comes from various ejaculations, is preserved at very low temperatures until the moment in the female cycle which is most conducive to fertilization.
Artificial insemination should not confuse us. It is, in reality, using the essential and natural elements of fertilization, the ovum and the sperm, and applying artificial technology. That is, the only thing that artificial techniques do is cooperate with the natural elements to overcome specific problems. The crude product of the life-giving cells is not substituted or changed in any way.
None of the techniques of assisted conception are entirely artificial. Neither the sperm nor the egg is created in the laboratory.
Man and Woman cannot be substituted. As the name implies, assisted conception is exactly that… assisted. These techniques can help lead to fertilization, but they do not replace the production of the ovum by the ovaries or the sperm by the testicles.
Old Techniques
Artificial Insemination of human beings has been practiced for many years in most developed countries. For example, in the United States, artificial insemination was carried out in 1890. Today, more than ten thousand births occur yearly in the United States using this technique.
Artificial Insemination by Husband (AIH)
This technique uses the sperm from the husband. The sperm is either placed in the wife’s vagina or injected into the uterus or the cervix.
Cases in which AIH is used:
This method is used when the man cannot deposit his sperm in the vagina in the usual way. This may be due to hypospadias, which is accentuated by some impotence. The technique can also overcome the problem of insufficient sperm. In this case, sperm is collected from various ejaculations.

Suppose the problem is that the cervix is impassable or that the vagina is inhospitable to the sperm. In that case, they are injected directly into the cervical channel or even further up so that the sperm has a chance of reaching and fertilizing the ovum.
In case of war
We want to add here that during World War II, the separation caused by the war was given as a reason:
North American soldiers fighting in the Pacific did not know when they would be given leave to return home because it was impossible to predict how many men were needed on active duty and for how long. Many of these young men were married and wished to have children.
Some decided to take advantage of AIH. Their semen was frozen and transported back to the United States. There the wives were artificially inseminated with the sperm from their husbands. A fair number of Americans can testify that they were conceived while their fathers risked their lives thousands of miles away.
Donor Insemination (DI)
artificial donor insemination consists of placing the sperm of a donor into the internal genital organs of a female who is not the donor’s wife. These sperm generally come from a sperm bank.
Application of DI:
This is sometimes incorrectly called heterologous artificial insemination. From a biological standpoint, it is homologous like the previous method since it unites two gametes from the same species. DI is used when the male spouse is sterile or when he is a carrier of a severe and indisputable hereditary disease. It is also used in the case of Rh incompatibility, which has caused various fetal deaths and other instances.
Precautions and Success Rates

To avoid possible blood-relatedness, a risk in small populations where the same donor could be the father to various children who later marry, there is a constant turnover of donors. The number of positive fertilizations by a single donor is also limited. In Spain, the maximum number stipulated by law is six.
Positive fertilization does not usually occur in more than ten percent of the cases in the first insemination. According to Dr. Pedro Caballero from the Hospital Ramón y Cajal of Madrid, Spain, there is an eighty percent success rate after the sixth insemination.
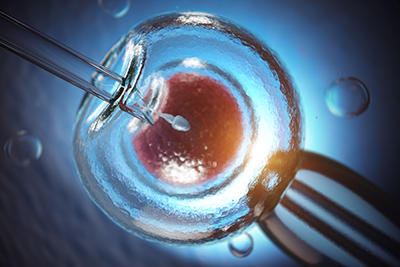
The Test Tube Baby (IVF)
In vitro fertilization (IVF) is placing the ovum and sperm in a container to produce fertilization. This type of fertilization is more accessible to accomplish when the man is under 40, and the woman is under 35. After these ages, fertility decreases.
Cases for IVF:
IVF is used in cases when, for one reason or another, the union of the female ovum with the male sperm cannot take place within the female genital system. Usually, there is a problem in the Fallopian tubes where the free circulation of the reproductive cells is not allowed, causing infertility.
This technique is also used when the fertilizing power of the husband’s sperm is low or when there is an unknown cause of sterility.
Pregnancies Without Ovaries
A woman who has her ovaries removed can become a mother. This was done by implanting one of the mother’s ova, extracted earlier, and then fertilized in vitro with the sperm from her husband. It has been done on various occasions.
The IVF Procedure
Ovum is produced by administering ovarian stimulants at the proper time in the female cycle. This stimulation causes one or more ova to be produced. All are collected. Once collected, they are placed in a container with a nutrient medium and kept in an incubator. They are later placed in contact with the male sperm.
With Only One Sperm:
Test-tube fertilization can occur with an insufficient number of sperm. A group of British scientists produced in vitro fertilization with only one sperm.
Embryos and Pre-embryos
When in vitro fertilization is successful, the egg or embryo begins to develop (pre-embryo is the term used in this case). After three days, the egg is placed in the woman’s uterine cavity, which will continue to grow if the pregnancy is successful.
The remaining pre-embryos can be preserved in a frozen state and may be used later. Legislation in some countries distinguishes between an embryo and a pre-embryo. It states that a pre-embryo is a fertilized egg whose development has not yet reached fourteen days.
The Spread of IVF
In 1978 Louise Brown, the first test-tube baby, was born in the United Kingdom. Until 1994, twenty thousand British children were produced through IVF. In the U.S., IVF was started in 1981. More than thirty thousand babies were born in fifteen years by this method. The first in vitro baby was born in France in 1982.
Validity if IVF
The number of implanted pre-embryos determines the success rate of in vitro pregnancies.
- With only one implantation, there is a 15 percent chance of successful pregnancy.
- When two are implanted, the success increases to twenty percent, with five percent leading to twins.
- Three implanted pre-embryos have a twenty-five percent success rate (fifteen percent individual pregnancies, eight percent twins, and two percent triplets).
The statistics are based on women under the age of 40. After the age of 40, these figures decrease. For example, in the case of implantation of only one pre-embryo, the pregnancy carries on successfully in only six percent of the cases if the woman is over 40 years of age, as opposed to fifteen percent of the cases of women under the age of 40. This is less than half the number of successes.
Prevention of Genetic Diseases
In vitro development, if the pre-embryo allows the egg to be punctured when it is made up of only eight cells to test one of them for certain deformations and diseases. Spanish law provides for the prevention and treatment of genetic or hereditary diseases as long as the treatment is carried out with sufficient diagnostic and therapeutic guarantees and as long as it takes place within the first fourteen days after fertilization (without counting the time in which the pre-embryo was preserved in a frozen state).
Freezing of pre-embryos:
This is done when there are more fertilized eggs than are desired. Multiple pregnancies occur when more than three are transplanted, and all prosper. This is not always desirable, and one or more of the pre-embryos are aborted. To avoid this problem, the leftover pre-embryos are frozen. These are used little by little until the mother becomes pregnant.
One or several can be implanted. The medical team treating the woman will determine the appropriate number that should be injected to obtain a pregnancy. Many children all over the world have been conceived from a frozen pre-embryo.
To evaluate this from an ethical perspective, we must have information about possible biological or genetic consequences; according to Withingam’s studies on rat embryos of eight cells, a source would have to remain frozen for between 200 and 1000 years before it would suffer any appreciable damage.
One of the problems created by this method is the destiny of the extra pre-embryos:
Do they remain frozen indefinitely? Are they destroyed? Are they used for experimentation?
There is significant variation in the legislation about frozen embryos. In some countries, after a few years, if not claimed, they belong to the bank holding then. In some cases, they can be used for research. In others, they must be destroyed. More than one hundred thousand embryos await their destiny in the United States. Some are protagonists of the parents’ highly publicized better legal battles, now divorced.
DISCLAIMER: All content on this website is presented solely for educational and informational objectives. Do not rely on the information provided as a replacement for advice, diagnosis, or treatment from a qualified medical expert. If you are pregnant, nursing, or have any preexisting medical concerns, talk to your doctor before using any herbal or natural medicines.
REFERENCES
- Isidro Aguilar, Doctor in Medicine and Surgery. “Encyclopedia of Health and Education for the Family.” Herminia Galbes, Doctor in Medicine and Surgery. Vols. 2: 276, 277, 278, 282, 283, 284 Print.
- Mayo Clinic: https://www.mayoclinic.org/tests-procedures/intrauterine-insemination/about/pac-20384722
- Human Reproduction Update (Journal). https://academic.oup.com/humupd
- American Society for Reproductive Medicine (ASRM). https://www.asrm.org