Here’s the honest answer most pages skip: the question of how to prevent allergies is really two questions wearing one phrase. One is whether you can stop an allergy from forming in the first place — and on that front the science has shifted dramatically in the past decade, mostly for babies. The other is how to keep the allergies you already have from making you miserable. Both have real answers. Neither is a permanent cure, and any page promising one is selling something.
So let’s keep them separate, because what protects a six-month-old is not what helps a 40-year-old with spring hay fever.
What “preventing allergies” actually means
An allergy is your immune system treating a harmless protein — tree pollen, a food, a pet’s dander — as if it were a threat. It releases histamine and other chemicals, and those produce the sneezing, itching, swelling, and congestion you feel. The tendency to react this way runs in families, which is why you can’t simply decide not to be allergic.
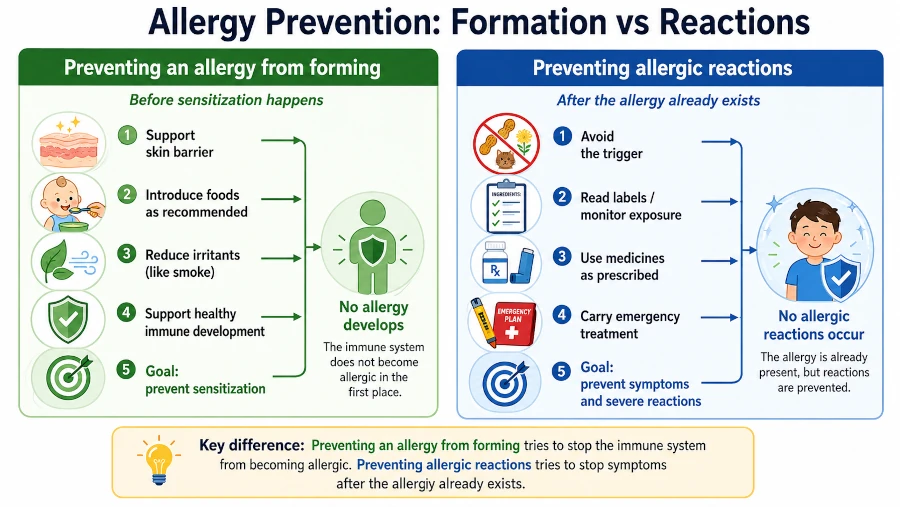
That gives “prevent” two meanings. The first is primary prevention: stopping an allergy from developing at all. The second is preventing reactions: keeping symptoms at bay once the allergy already exists. The old line that “there’s nothing you can do” is wrong on both counts — but the leverage you have is different for each.
Can you stop an allergy from forming?
In babies: early food introduction changed everything
For years, parents were told to delay giving infants allergenic foods like peanut. That advice turned out to be backwards.

In the landmark LEAP trial, regularly feeding peanut to infants from early life cut the rate of peanut allergy at age five by about 81% compared with avoiding it [NIAID, 2017]. Follow-up showed the protection lasted into adolescence, even when children weren’t eating peanut consistently every year [NIAID, 2024].
On the strength of those results, the National Institute of Allergy and Infectious Diseases recommended that peanut — in a developmentally safe form, never whole nuts — be introduced for most infants around 4 to 6 months and then kept in the diet, with a target of roughly 2 grams of peanut protein about three times a week [NIAID, 2017]. The same “introduce early, don’t delay” approach applies to egg.
One important exception: infants with severe eczema, an existing egg allergy, or both are at higher risk for peanut allergy and should be evaluated — often with testing — before their first taste of peanut [NIAID, 2017]. If that’s your baby, talk to your pediatrician or an allergist first rather than introducing peanut at home.
Two worries, settled: there’s no benefit to a mother avoiding allergenic foods during pregnancy or breastfeeding to protect the baby, and breastfeeding itself doesn’t determine whether a child develops a food allergy [AAAAI]. And this isn’t theory — since the guidelines took hold, U.S. rates of peanut and overall food allergy have measurably declined [AAP, 2025].
In adults: be honest about what’s possible
Once you’re grown, you can’t reliably stop a new allergy from forming through diet, supplements, or “immune-boosting” products — the evidence for that isn’t there. What you can do is shift your energy to the second question: preventing reactions. That’s where adults have real control.
How to prevent allergies when you already have allergies
Get an actual diagnosis first
You can’t avoid or treat a trigger you haven’t identified. An allergist can pin down what you actually react to using your history plus skin or blood testing — which often surprises people who’ve been blaming the wrong thing. Guessing tends to mean money spent on fixes that were never going to work.
Reduce exposure where it’s realistic
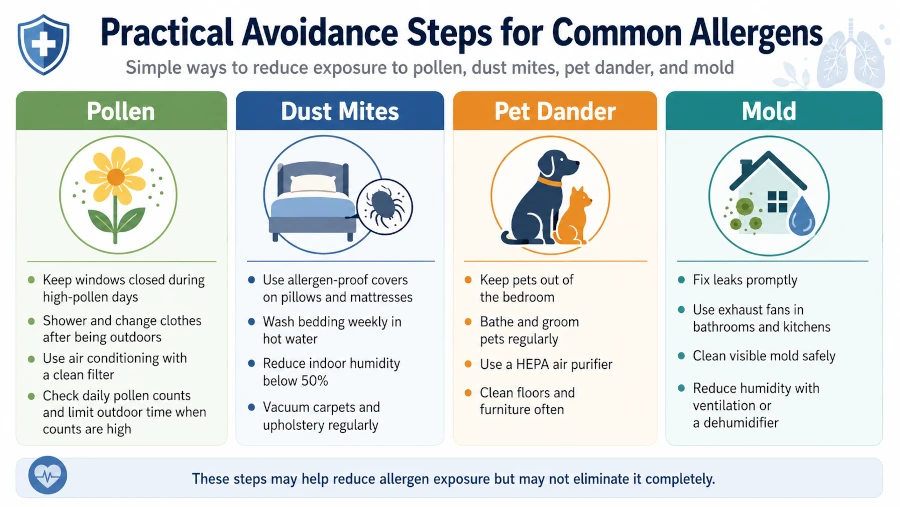
Avoidance is the first move with no side effects. The catch is that only some allergens are practically avoidable, and single tactics often help less than people hope — bundles of measures tend to work better than any one trick.
| Trigger | What actually helps | Reality check |
| Pollen | Track local counts; keep windows shut on high days; shower and change after being outdoors; dry laundry inside | You can’t avoid outdoor air — aim to lower exposure on peak days, not eliminate it |
| Dust mites | Allergen-proof mattress and pillow covers; wash bedding weekly in hot water; keep indoor humidity 30–50%; cut clutter and carpet | Evidence for any single step is modest; combining them works better |
| Pet dander | Keep pets out of the bedroom; use HEPA filtration; wash hands after contact | Rehoming is rarely necessary; reducing bedroom exposure helps most |
| Mold | Fix leaks promptly; control bathroom and basement humidity; clean visible mold; keep AC filters clean | Damp filters can harbor mold and worsen symptoms — maintain them |
Use the right medication, the right way
This is where a lot of people leave relief on the table by reaching for the wrong product.
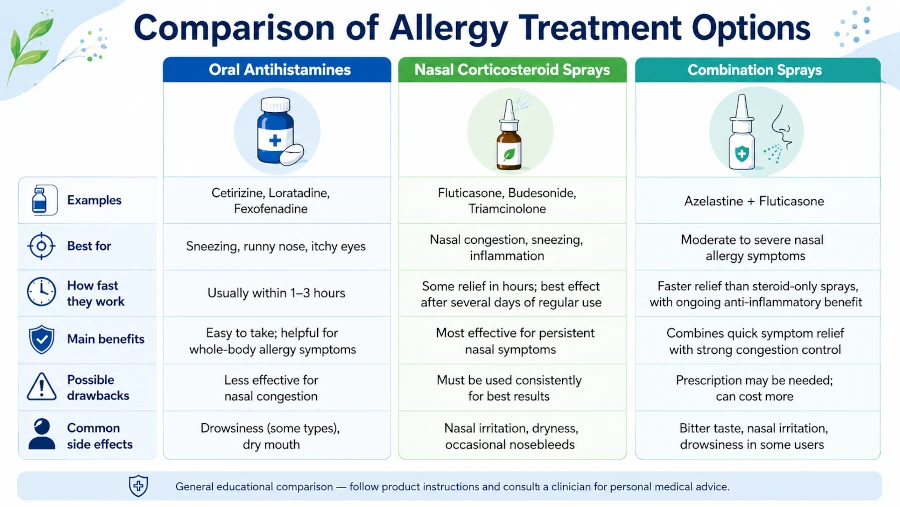
| Option | Best for | Worth knowing |
| Second-generation oral antihistamines (cetirizine, loratadine, fexofenadine) | Sneezing, itching, runny nose, hives | Preferred over older first-generation types (like diphenhydramine), which cause drowsiness and impair driving; cetirizine still makes some people mildly sleepy [AAAAI/ACAAI, 2020] |
| Intranasal corticosteroid sprays (fluticasone, mometasone, triamcinolone) | Nasal congestion and overall nasal symptoms | The single most effective treatment for nasal allergy symptoms — more effective than oral antihistamines for congestion. Works best used daily and takes a few days to reach full effect, so start before your peak season [AAAAI/ACAAI, 2020] |
| Combination nasal spray (intranasal antihistamine + steroid) | Symptoms that don’t settle on one drug | Adds benefit when a steroid alone isn’t enough [AAAAI/ACAAI, 2020] |
| Decongestants | Short-term congestion relief | Topical sprays used more than 3 days cause rebound congestion; oral versions can raise blood pressure — short-term only |
| Montelukast | An add-on option | Carries a U.S. boxed warning for mood and behavior changes; generally not a first choice [AAAAI/ACAAI, 2020] |
A practical tip that costs nothing: if you know your season, start your nasal steroid a week or two before pollen peaks rather than waiting until you’re already congested.
Consider immunotherapy — the closest thing to changing the allergy itself
Medications mask symptoms. Allergen immunotherapy is the one approach that actually retrains the immune response. It comes in two forms: subcutaneous immunotherapy (SCIT, the classic “allergy shots”) and sublingual immunotherapy (SLIT, under-the-tongue tablets or drops). Given over roughly three to five years, it can meaningfully reduce symptoms and the medication you need — and the benefit can persist after you stop treatment [Allergen Immunotherapy review, 2024].
The trade-offs are practical. Allergy shots carry a small risk of serious reactions, so they’re given in a medical office with monitoring. SLIT tablets — available for grass, ragweed, and dust mite — can be taken at home after a supervised first dose. It’s worth raising with an allergist if avoidance and daily medication aren’t enough, or if you’d rather not medicate indefinitely.
When an allergic reaction is an emergency
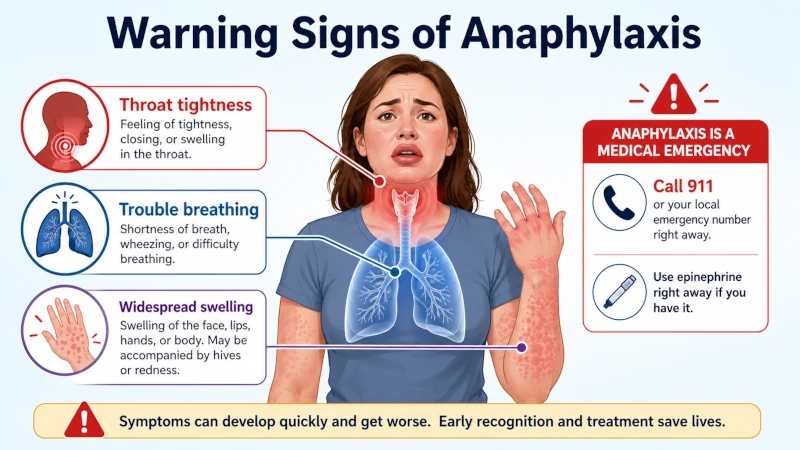
Most allergies are miserable, not dangerous. But some reactions — usually to foods, insect stings, medications, or latex — can escalate into anaphylaxis, which is life-threatening and moves fast.
Call for help if you see several of these at once: trouble breathing or wheezing, tightness in the throat, widespread hives or swelling, swelling of the lips, tongue, or throat, vomiting or diarrhea alongside other symptoms, dizziness or feeling faint, or a sudden sense that something is very wrong [ACAAI, 2025; Mayo Clinic, 2025].
If you carry epinephrine, use it immediately into the outer thigh — don’t wait to see whether the reaction passes, and don’t reach for an antihistamine instead. Antihistamines can’t reverse airway swelling or low blood pressure, and the delay can be dangerous [ACAAI, 2025]. After using epinephrine, get emergency care; call 911 if symptoms are severe, don’t fully resolve, or return after the first dose [JTFPP, 2023]. Carry two doses, since a second is sometimes needed.
For non-urgent help, see an allergist if symptoms disrupt your sleep or daily life, over-the-counter medicine isn’t cutting it, you’re unsure what you react to, or you’ve ever had a severe reaction.
Who should take extra care
- Pregnant or breastfeeding: Several allergy medicines are used during pregnancy, but confirm choices with your clinician. Immunotherapy generally isn’t started during pregnancy, though continuing an established course may be fine — ask.
- Anyone driving or operating machinery: Avoid first-generation, sedating antihistamines.
- Older adults or people with high blood pressure or heart conditions: Use decongestants cautiously, if at all.
- Children: The early-introduction guidance above applies; a clinician should set any dosing and device choices.
- People with poorly controlled asthma: A reason to get care, and a caution before starting immunotherapy.
| Health Disclaimer This article is for general education and information only. It is not a substitute for diagnosis, treatment, or advice from a qualified healthcare professional who knows your history. Allergy medications and immunotherapy carry individual risks and interactions. If you are pregnant, breastfeeding, managing another medical condition, or considering treatment for a child, talk with your doctor or a board-certified allergist before acting on anything here. If you have signs of a severe allergic reaction (anaphylaxis), use prescribed epinephrine and seek emergency care immediately. |
Frequently Asked Questions
Can allergies be cured permanently?
No treatment permanently erases the underlying tendency. Immunotherapy comes closest — over three to five years it can produce lasting relief that continues after you stop.
Do allergies ever go away on their own?
Some childhood food allergies, such as milk and egg, are commonly outgrown. Environmental allergies can change across your life but often persist, which is why management matters.
My baby is older than six months — is it too late to introduce peanut?
No. Early is better, but later introduction still counts. Talk to your pediatrician first if your baby has severe eczema or an egg allergy.
Can I prevent seasonal allergies before the season starts?
You can blunt them. Starting an intranasal corticosteroid a week or two before your pollen season, and cutting exposure on high-count days, works better than waiting until symptoms peak.
Do natural remedies like local honey or supplements prevent allergies?
The evidence is weak and inconsistent. They’re not a reliable substitute for proven avoidance, medication, or immunotherapy.
What’s the difference between a food allergy and a food intolerance?
An allergy is an immune reaction that can become life-threatening; an intolerance (like lactose intolerance) is a digestive problem that’s uncomfortable but not dangerous in the same way.
References
- NIAID. Addendum Guidelines for the Prevention of Peanut Allergy in the United States (2017). View source
- NIAID / NIH. Introducing Peanut in Infancy Prevents Peanut Allergy into Adolescence (2024). View source
- American Academy of Pediatrics, Pediatrics. Encouraging Trends in Peanut Allergy Prevention (2025). View source
- AAAAI/ACAAI Joint Task Force. Rhinitis 2020: A practice parameter update, J Allergy Clin Immunol. View source
- AAAAI/ACAAI. Treatment of Seasonal Allergic Rhinitis guideline summary, AAFP (2018). View source
- Allergen Immunotherapy: Evidence for SCIT and SLIT, JACI: In Practice (2024). View source
- JTFPP. Anaphylaxis: A 2023 practice parameter update, Ann Allergy Asthma Immunol. View source
- ACAAI. Anaphylaxis — Symptoms & Treatment (reviewed 2025). View source
- ACAAI. Epinephrine Auto-Injector (updated 2026). View source
- Mayo Clinic. Anaphylaxis — Diagnosis & Treatment (2025). View source