Contents
- 1 Quick Refresher: What Ulcerative Colitis Does to the Gut
- 2 The Core Principle: Match Your Diet to the Phase You’re In
- 3 What to Eat During a Flare
- 4 What to Eat During Remission: A Mediterranean-Style Pattern
- 5 Foods to Limit Regardless of Phase
- 6 Supplements: What the Evidence Actually Supports
- 7 Practical Strategies That Actually Help
- 8 Who Should Be Especially Cautious With Restrictive Diets
- 9 When Diet Is Not Enough: Red Flags to Take Seriously
- 10 Realistic Expectations
- 11 Frequently Asked Questions
- 12 References

A diet for ulcerative colitis cannot cure the disease, but the right food choices can lower symptom burden, reduce flare frequency, and protect long-term nutrition. Ulcerative colitis (UC) is a chronic inflammatory bowel disease that affects the lining of the colon and rectum, and what you put on your plate becomes part of how your gut behaves day to day. There is no single ulcerative colitis diet that fits everyone. But the research points to clear patterns: a Mediterranean-style way of eating during remission, a gentler low-residue pattern during active flares, and careful attention to your personal triggers.
This guide walks through what to eat in remission, what to switch to during a flare, which trigger foods to limit, and which supplements have actual evidence behind them. It also covers when food is no longer enough and you need a clinician. [NIDDK, 2024] [Crohn’s & Colitis Foundation, 2026]
Quick Refresher: What Ulcerative Colitis Does to the Gut
UC causes continuous inflammation and ulcers in the colon and rectum. Common symptoms include bloody diarrhea, urgency, abdominal cramps, fatigue, and unintended weight loss. The disease tends to cycle through periods of active flare and periods of remission, and food choices interact differently with each phase. Diet does not cause UC, but it can either calm or aggravate inflammation in a colon that is already vulnerable. [NIDDK, 2024]
The Core Principle: Match Your Diet to the Phase You’re In
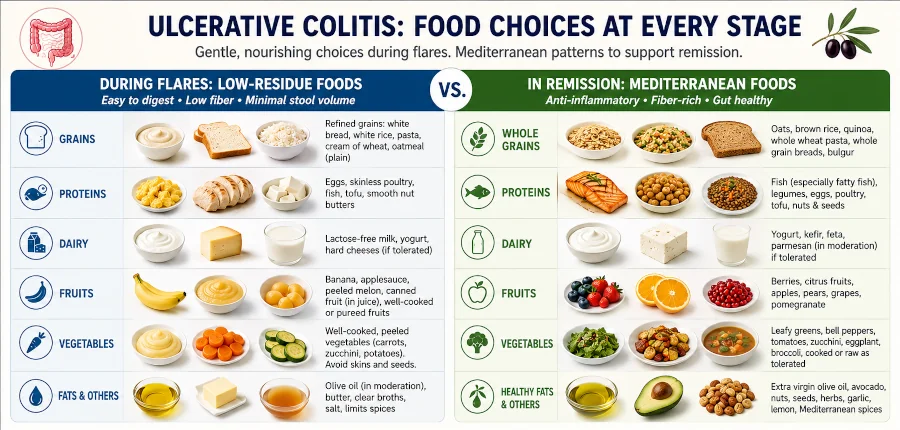
Two patterns matter most. During an active flare, the goal is to eat foods that are easy on an inflamed colon — soft, low-fiber, low-fat, simple. During remission, the goal flips: bring back fiber, plants, fish, and olive oil to keep inflammation down and nutrition complete. The Crohn’s & Colitis Foundation puts it plainly: try to keep the diet as expansive as possible, especially with tolerated plant-based foods, and only restrict when symptoms demand it. [Crohn’s & Colitis Foundation, 2026]
Here is a quick side-by-side:
| Focus | During an active flare | During remission |
| Fiber | Low (peeled, cooked, refined) | Normal to high, as tolerated |
| Texture | Soft, moist, well cooked | Whole foods, varied textures |
| Fat | Lower; avoid fried | Unsaturated fats (olive oil, fish, nuts) |
| Meals | 5–6 small, spaced out | 3 meals + snacks as needed |
| Fluids | Water, broth, oral rehydration | Water as a default; limit alcohol |
What to Eat During a Flare

A short-term low-fiber or low-residue diet is the most common adjustment during active disease. The aim is fewer, smaller stools, less cramping, and more rest for the colon lining. It is not a long-term solution, and it should not replace medication. [Mayo Clinic, 2024]
Foods that usually sit well during a flare
- White rice, refined pasta, white bread, oatmeal, and cream of wheat
- Ripe bananas, applesauce, melon, and canned peaches in juice
- Peeled, cooked vegetables — carrots, zucchini, squash, potatoes without skin
- Lean protein — skinless chicken, turkey, eggs, baked fish, tofu
- Smooth nut butters (in small amounts) if whole nuts trigger symptoms
- Low-fat yogurt or kefir, if dairy is tolerated; lactose-free options if not
- Bone broth and clear broths for hydration and sodium during heavy diarrhea
Foods most people limit during a flare
- Raw cruciferous vegetables — broccoli, cabbage, Brussels sprouts, cauliflower
- Nuts, seeds, popcorn, corn, and dried fruit
- Fatty, fried, or heavily spiced foods
- Carbonated drinks, alcohol, and large amounts of caffeine
- Dairy if it causes pain, gas, or diarrhea — lactose intolerance is more common during flares [Mayo Clinic, 2024]
Keep portions small and meals frequent. Five or six modest meals tend to be easier on a tender colon than two or three large ones. [Crohn’s & Colitis Foundation, 2026]
What to Eat During Remission: A Mediterranean-Style Pattern
Once symptoms quiet down, the priority becomes long-term gut health and nutrition. The strongest evidence here points to a Mediterranean dietary pattern — vegetables, fruit, legumes, whole grains, fish, olive oil, and modest dairy, with limited red and processed meat. In a 2023 randomized controlled trial published in the Journal of Crohn’s and Colitis, adults with UC in remission who followed a Mediterranean pattern for 12 weeks had lower fecal calprotectin (a marker of gut inflammation) and a healthier microbiome than those on a Canadian habitual diet. At week 12, only 20% of the Mediterranean group had calprotectin above 100 µg/g, versus 75% of the comparison group. [Haskey et al., 2023]
A broader 2023 systematic review reached a similar conclusion: Mediterranean, low-FODMAP, and anti-inflammatory dietary patterns can improve symptoms and quality of life in UC, though the certainty of evidence remains moderate. [Abbas et al., 2023] A larger narrative review in Gastroenterology Clinics of North America also concluded that diets low in animal protein and higher in fiber help maintain remission in UC, with the caveat that personalization matters. [Damas, 2022]

What a Mediterranean week looks like
- Vegetables and fruit at most meals — aim for variety and color
- Whole grains such as oats, barley, brown rice, and whole wheat
- Beans, lentils, and chickpeas a few times a week, if tolerated
- Fatty fish (salmon, sardines, mackerel) two to three times a week
- Olive oil as the main cooking fat; nuts and seeds as snacks
- Yogurt or kefir if dairy is comfortable; otherwise unsweetened plant alternatives
- Red meat occasional rather than daily; minimize processed meat
Foods to Limit Regardless of Phase
Some dietary patterns are consistently linked with worse outcomes in inflammatory bowel disease, no matter where you are in the disease cycle. The International Organization for the Study of IBD (IOIBD) recommends limiting saturated fat (full-fat dairy, palm oil, coconut oil in large amounts), red meat, processed meat, and emulsifiers such as carboxymethylcellulose and polysorbate-80, both found in many ultra-processed foods. [Damas, 2022]
- Ultra-processed snack foods, fast food, and sugary drinks
- Processed meats — hot dogs, deli meats, sausages, bacon
- Excess alcohol
- Trans fats and large amounts of fried food
- Artificial sweeteners and emulsifiers in processed foods, where you can spot them on labels

Supplements: What the Evidence Actually Supports
UC is a high-stakes condition, so honest evidence labeling matters here. Most of the supplements marketed for colitis have either weak evidence, mixed evidence, or evidence limited to specific situations. A short tour:
| Supplement | Evidence level | What the research shows |
| Omega-3 / fish oil | Mixed to negative | A Cochrane review of three trials (138 patients) found no benefit for maintaining UC remission compared with placebo. |
| Probiotics (general) | Limited | Some strains, especially VSL#3-type formulations and E. coli Nissle 1917, may help maintain remission in mild-to-moderate UC. Not all probiotics work the same. |
| Curcumin (turmeric extract) | Promising but early | Small RCTs suggest curcumin added to standard therapy may help maintain remission. Dosing varies and quality of trials is uneven. |
| Vitamin D | Correct deficiencies | Low vitamin D is common in UC. Replacement when deficient is sensible; routine high-dose supplementation in everyone is not. |
| Iron | When indicated | Iron deficiency anemia is frequent due to blood loss. Oral or IV iron should be guided by a clinician. |
| Aloe vera (oral gel) | Limited | One small trial reported clinical improvement in active UC, but the evidence base is thin and oral aloe can have safety issues. |
The fish oil finding tends to surprise people, because supplements get marketed around inflammation. A Cochrane systematic review concluded that omega-3 fatty acids were safe but did not reduce relapse in UC remission. [Cochrane, 2014] That is not a reason to avoid fatty fish in your diet — whole-food fish remains a Mediterranean staple — it is a reason to be skeptical of fish oil capsules sold as a UC treatment.
Talk with a gastroenterologist or a registered dietitian who specializes in IBD before starting any supplement, especially during pregnancy, breastfeeding, or while on biologics or immunosuppressants.
Practical Strategies That Actually Help
Keep a food and symptom diary
Trigger foods are individual. Two people with UC can react to completely different things. A simple notebook — what you ate, when, how you felt over the next 24 hours — usually surfaces patterns within two or three weeks. Bring it to your dietitian appointment. [Crohn’s & Colitis Foundation, 2026]
Eat smaller meals more often
Five or six small meals tend to feel better than two or three large ones, especially during a flare. Smaller portions reduce post-meal urgency and gas.
Pay attention to hydration
Diarrhea and blood loss both drain fluids and electrolytes. Aim for water throughout the day and add oral rehydration solutions or low-sugar electrolyte drinks if symptoms are heavy. Coconut water and broth-based soups are useful.
Cook simply
Steaming, baking, grilling, and stewing tend to be gentler than frying. Peeling fruits and vegetables and removing seeds further reduces residue during flares.
Work with an IBD dietitian if you can
A registered dietitian who specializes in IBD can build a personalized plan, screen for nutrient gaps (iron, B12, folate, calcium, vitamin D), and help you reintroduce foods safely after a flare. This is the single highest-yield intervention most patients are not yet using.
Who Should Be Especially Cautious With Restrictive Diets
- Children and teens — restriction risks growth and development gaps
- Pregnant or breastfeeding people — nutrient needs increase
- Anyone underweight or losing weight unintentionally
- People on multiple medications, since some interact with grapefruit, calcium, or fiber timing
- Anyone considering very-low-fiber or carnivore-style diets long-term — these are not supported by evidence in UC and may harm the microbiome
When Diet Is Not Enough: Red Flags to Take Seriously
Call your gastroenterologist or seek urgent care if you have any of the following:
- Six or more bloody stools per day
- Persistent fever or shaking chills
- Severe abdominal pain or a bloated, distended belly
- Rapid heart rate, dizziness, or signs of dehydration
- Unintended weight loss of more than 5% of body weight
- Black, tarry stools or large amounts of fresh blood
These can signal severe disease activity, including toxic megacolon, which is a medical emergency. Diet is part of UC management — never a substitute for medication, monitoring, or surgery when needed. [NIDDK, 2024]
Realistic Expectations
Diet changes work best when they are sustained and combined with appropriate medical care. Most people notice meaningful symptom improvement within 4 to 12 weeks of consistent dietary change, but timelines vary widely. Food will not replace mesalamine, biologics, or other UC therapies your clinician prescribes. A reasonable goal is fewer flares, better day-to-day comfort, stronger nutrition, and a calmer relationship with food — not a cure.
If irritable bowel symptoms persist between flares, a low-FODMAP trial can help. Many of the same principles overlap with what works in IBS-friendly eating, though UC has its own inflammatory layer that food alone does not address.
| Health Disclaimer This article is for educational purposes only and does not replace medical advice, diagnosis, or treatment from a qualified healthcare professional. Ulcerative colitis is a serious chronic condition. Do not stop or change prescribed medications based on dietary information. Talk with your gastroenterologist or a registered dietitian who specializes in inflammatory bowel disease before making major changes to your diet, especially during a flare, during pregnancy or breastfeeding, or while on biologics or immunosuppressants. If you experience severe abdominal pain, heavy rectal bleeding, persistent fever, signs of dehydration, or rapid weight loss, seek urgent medical care. |
Frequently Asked Questions
Is there a single best diet for ulcerative colitis?
No. The best-supported pattern for remission is a Mediterranean-style diet, and the most common adjustment during a flare is a temporary low-residue diet. Beyond that, food triggers are individual, which is why a food diary and a dietitian are more useful than any one named diet.
Should I avoid fiber if I have UC?
Not in general. Restrict fiber during active flares — peel and cook vegetables, choose refined grains, avoid nuts and seeds — then bring fiber back as you enter remission. Long-term low-fiber diets are linked with worse microbiome diversity and are not recommended.
Does fish oil help ulcerative colitis?
The supplement form does not reliably maintain remission, based on a Cochrane review. Eating fatty fish two to three times a week as part of a Mediterranean pattern is still a reasonable choice for general health and nutrition.
Can dairy trigger UC flares?
Sometimes. Lactose intolerance is more common during active disease, and full-fat dairy contributes saturated fat that the IOIBD recommends limiting. Many people tolerate yogurt, kefir, and hard cheeses better than fluid milk.
Is the autoimmune protocol (AIP) diet useful for UC?
Small pilot studies show some benefit, but the evidence is weak and AIP is highly restrictive. It is reasonable to try short-term under a dietitian’s supervision; it is not reasonable to follow long-term without guidance, given the risk of nutrient gaps.
References
- National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Ulcerative Colitis. NIH, 2024. → View source
- Crohn’s & Colitis Foundation. What Should I Eat With Crohn’s Disease or Ulcerative Colitis? Updated 2026. → View source
- Crohn’s & Colitis Foundation. Special IBD Diets. Accessed 2026. → View source
- Mayo Clinic. Ulcerative colitis flare-ups: 5 tips to manage them. Updated 2024. → View source
- Turner D, Shah PS, Steinhart AH, et al. Omega 3 fatty acids (fish oil) for maintenance of remission in ulcerative colitis. Cochrane Database of Systematic Reviews, CD006443. → View source
- Haskey N, Estaki M, Ye J, et al. A Mediterranean Diet Pattern Improves Intestinal Inflammation Concomitant with Reshaping of the Bacteriome in Ulcerative Colitis: A Randomised Controlled Trial. J Crohns Colitis. 2023;17(10):1569–1578. doi:10.1093/ecco-jcc/jjad073 → View source
- Abbas N, Shakil M, Rana ZA, et al. A Systematic Review of the Role of Diet in Ulcerative Colitis. Cureus. 2023;15(5):e39350. doi:10.7759/cureus.39350 → View source
- Damas OM, Garces L, Abreu MT. Diet as treatment for inflammatory bowel disease: recommendations from the latest evidence. Gastroenterol Clin North Am. 2022;51(2):353–374. → View source