
Energy boosting supplements can help in specific situations, but most healthy adults who feel tired do not need them. Persistent low energy is usually a signal — about sleep, diet, stress, medication, or an undiagnosed condition like iron-deficiency anemia or low thyroid function. Supplements only do real work when there is a measurable gap to fill. [Harvard Health, 2024]
This guide covers seven of the most studied options — coenzyme Q10, iron, vitamin B12, vitamin D, magnesium, ashwagandha, creatine, and caffeine — what the evidence shows for each, who is most likely to notice a difference, realistic doses, and the safety issues your doctor or pharmacist would want you to know about before you start.
When a Supplement Actually Helps With Energy
The honest answer from the research: correcting a real deficiency tends to work; topping up someone who is not deficient usually does not. Harvard Medical School puts it plainly — if your levels of a given nutrient are already normal, taking more will not raise your energy. [Harvard Health, 2024]
Before reaching for a bottle, check the obvious causes first:
- Sleep — most adults need 7 to 9 hours; chronic short sleep is the single biggest energy thief.
- Diet — skipping meals, very low-carb crash diets, and ultra-processed snacks cause blood-sugar swings that feel like fatigue.
- Hydration and caffeine timing — too little water or caffeine after 2 p.m. both backfire.
- Medications — blood-pressure drugs, antihistamines, antidepressants, opioids, and some statins commonly list fatigue as a side effect.
- Underlying conditions — iron-deficiency anemia, thyroid disorders, depression, sleep apnea, diabetes, and post-viral fatigue can all present as “just being tired.”
If fatigue has lasted more than a few weeks despite reasonable sleep and food, get bloodwork before self-treating. A basic panel (CBC, ferritin, TSH, vitamin D, B12) often reveals the real cause. For a deeper look at lingering tiredness after illness, see natural remedies for post-COVID fatigue.
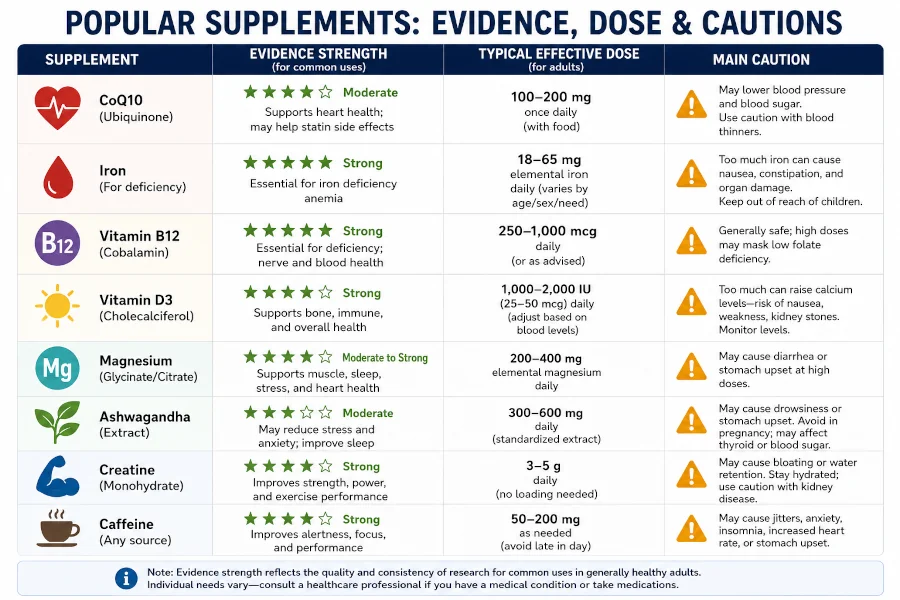
Quick Comparison: Seven Energy Boosting Supplements at a Glance
Evidence strength uses a simple scale: Strong = consistent human trials, including meta-analyses; Moderate = several positive randomized trials but mixed results overall; Limited = small studies, narrow populations, or mostly observational data.
| Supplement | Best for | Evidence | Typical adult dose | Main caution |
| CoQ10 | People with diagnosed deficiency, statin users, chronic fatigue | Moderate | 100–200 mg/day | May interact with warfarin and blood-pressure medications |
| Iron | Confirmed iron-deficiency anemia | Strong (when deficient) | Per blood-test results, usually 18–65 mg elemental iron | Toxic in overdose; never supplement without testing |
| Vitamin B12 | Vegans, older adults, people on metformin or acid-reducers | Strong (when deficient) | RDA 2.4 mcg; supplements often 100–1,000 mcg | Generally safe; high doses are excreted in urine |
| Vitamin D | Low blood 25-OH vitamin D, limited sun exposure | Moderate (when deficient) | RDA 600–800 IU; deficiency dosing 1,000–2,000 IU/day | Upper limit 4,000 IU/day; toxicity at chronic high doses |
| Ashwagandha | Stress-driven fatigue, poor sleep | Limited to moderate | 250–600 mg/day root extract, 8–12 weeks | Rare reports of liver injury; avoid in pregnancy and thyroid disease |
| Creatine monohydrate | High-intensity exercise, strength training | Strong (for performance, not general fatigue) | 3–5 g/day | Generally safe; check with doctor if kidney disease |
| Caffeine | Short-term alertness, pre-workout focus | Strong | Up to 400 mg/day for healthy adults (FDA) | Anxiety, palpitations, sleep disruption; less for pregnancy |
Coenzyme Q10 (CoQ10)
CoQ10 is a compound your cells use to produce ATP — the molecule that powers nearly everything your body does. Levels fall with age and with certain medications, especially statins, which can leave some users feeling sluggish or weak. A 2022 meta-analysis of 13 randomized trials with 1,126 participants found CoQ10 supplementation produced a small but statistically significant reduction in fatigue scores compared with placebo, with greater effect at higher doses and longer treatment durations. [Tsai et al., 2022]
Who tends to benefit: Statin users with muscle fatigue, people with diagnosed mitochondrial conditions, and those recovering from heart failure under medical supervision. Healthy young adults with normal energy rarely notice a difference.
Typical dose: 100 to 200 mg per day, taken with a meal containing fat for better absorption.
Safety: Generally well tolerated. CoQ10 can interact with warfarin (reducing its effect) and with some blood-pressure and chemotherapy drugs — check with your prescriber first.
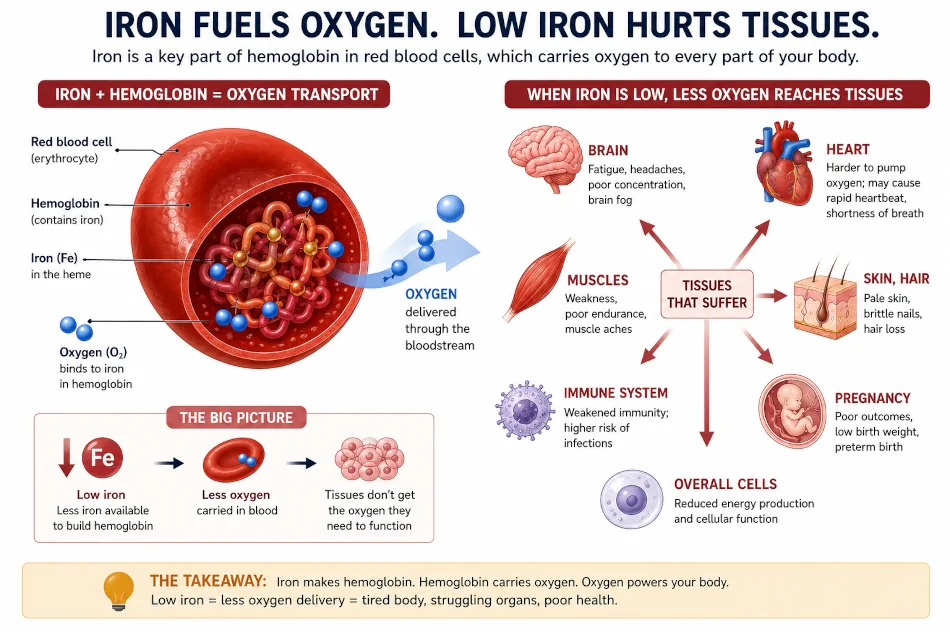
Iron
Iron carries oxygen on hemoglobin in your red blood cells. When iron stores fall low enough, the result is iron-deficiency anemia — and the most reliable early symptom is exhausting, persistent fatigue that does not improve with rest. Mayo Clinic also lists pale skin, shortness of breath on exertion, cold hands and feet, headaches, brittle nails, and unusual cravings for ice or non-food items. [Mayo Clinic, 2025]
Who tends to benefit: People with confirmed low ferritin or anemia — most commonly women with heavy periods, pregnant women, vegetarians and vegans, frequent blood donors, athletes (especially long-distance runners), and anyone with gastrointestinal blood loss.
Why testing first matters: Iron is the one nutrient on this list where blind supplementation is actively risky. Too much iron is stored in the liver and other organs and can cause damage. The NIH Office of Dietary Supplements stresses that healthy adults already meeting their RDA gain nothing from extra iron and may be harmed by it. [NIH ODS, 2023]
Food first: Many people can correct mild deficiency through diet alone. See our guide to iron-rich foods and our list of foods that help with anemia. Pair plant-based (non-heme) iron with vitamin C — for example, spinach with citrus or peppers — to roughly triple absorption.
Typical dose: Adults with anemia are usually started on 18 to 65 mg elemental iron per day under medical supervision, often as ferrous sulfate or ferrous bisglycinate (better tolerated). Many people now do best with every-other-day dosing, which improves absorption and cuts side effects.
Side effects: Constipation, dark stools, nausea, and stomach pain are common. Take with vitamin C and food (but not with calcium, coffee, or tea, which block absorption).
Vitamin B12
B12 helps make red blood cells and keeps the nervous system running. Without enough, you can develop megaloblastic anemia — a blood condition that causes weakness, tiredness, and tingling in the hands or feet. [NIH ODS, 2024]
Who tends to benefit: Strict vegetarians and vegans (B12 occurs naturally only in animal foods), adults over 50 (absorption declines with age), people on long-term metformin or proton-pump inhibitors like omeprazole, and anyone with pernicious anemia, celiac disease, or Crohn’s. A 2016 review noted that even mild B12 insufficiency can affect cognitive sharpness and energy long before classic anemia appears. [Kennedy, 2016]
Typical dose: The RDA is just 2.4 mcg per day for adults. Over-the-counter supplements often contain 100 to 1,000 mcg because absorption is inefficient — the body takes what it needs and discards the rest in urine. Sublingual tablets and oral tablets work equally well for most people; injections are reserved for severe deficiency or absorption disorders.
Realistic expectation: If you are truly deficient, energy can improve within weeks. If you are not deficient, extra B12 will not make you more alert — that is one of the most consistent findings in the energy-supplement literature.
Vitamin D
Vitamin D is unusual: your skin makes it from sunlight, and very few foods contain it naturally. Deficiency is widespread — NHANES data show roughly a quarter of U.S. adults have inadequate blood levels. [NIH ODS, 2024] Symptoms tend to be vague — muscle weakness, low mood, bone aches, and a general lack of stamina.
Who tends to benefit: People who get limited sun (indoor workers, northern climates, regular sunscreen users), those with darker skin, older adults, people with obesity, and anyone with malabsorption conditions. The simplest way to know if you need it is a 25-hydroxyvitamin D blood test.
Typical dose: The RDA is 600 IU for most adults and 800 IU for those over 70. Correcting a measured deficiency usually involves 1,000 to 2,000 IU per day, occasionally higher under a doctor’s supervision. The tolerable upper limit is 4,000 IU per day for adults. Vitamin D is fat-soluble, so take it with a meal that contains some fat.
Cautions: Toxicity is rare but possible with long-term very high doses — symptoms include nausea, constipation, weakness, and elevated blood calcium. Check with your doctor if you take thiazide diuretics, digoxin, or have a history of kidney stones.
Vitamin D also supports immune function, which is one reason a true deficiency can leave you feeling rundown in ways that look like simple fatigue.
Magnesium
Magnesium is involved in more than 300 enzyme reactions, including the one that converts food into usable energy. Harvard Health notes that roughly half of U.S. adults consume less magnesium than they need from food, and low intake has been linked to fatigue, muscle cramps, and poor sleep — all of which feed into low daytime energy. [Harvard Health, 2024]
Who tends to benefit: People with low dietary intake (few leafy greens, beans, nuts, or whole grains), heavy drinkers, people on long-term proton-pump inhibitors or diuretics, and those with type 2 diabetes.
Typical dose: RDA is 310 to 420 mg per day depending on age and sex. Supplemental doses for adults are usually 200 to 400 mg per day. Magnesium glycinate and citrate are better absorbed and gentler on the gut than magnesium oxide, which is often used because it is cheap but absorbs poorly.
Side effects: Loose stools at high doses (especially with oxide and citrate forms). Avoid high-dose magnesium if you have advanced kidney disease.
Ashwagandha
Ashwagandha (Withania somnifera) is an adaptogenic herb used in Ayurvedic medicine for centuries. The National Center for Complementary and Integrative Health states that some preparations may be effective for stress and insomnia, but evidence for anxiety is unclear and long-term safety has not been well established. [NCCIH, 2023] Because much fatigue in modern life is stress-driven, this is where ashwagandha may indirectly help: by lowering cortisol and improving sleep, it can take the edge off the kind of tiredness that lingers even after a full night in bed.
A 2020 systematic review and meta-analysis in Nutrients found ashwagandha supplementation modestly improved VO2max — a measure of cardiorespiratory endurance — in healthy adults and athletes, suggesting some real exercise-capacity benefit. [Pérez-Gómez et al., 2020] For more context on this category, see our guide to adaptogenic herbs.
Typical dose: 250 to 600 mg per day of a standardized root extract, often taken in two divided doses, for 8 to 12 weeks. Standardized extracts (such as KSM-66 or Sensoril) are more consistent than raw powders.
Cautions: Avoid during pregnancy and breastfeeding. Use caution if you have an autoimmune condition (lupus, rheumatoid arthritis, Hashimoto’s), thyroid disease, or are on sedatives, thyroid medication, or immunosuppressants. Rare cases of liver injury have been reported in the medical literature — stop and see a doctor if you develop yellowing of the skin or eyes, dark urine, or upper-right abdominal pain.
Creatine Monohydrate
Creatine is one of the most-studied supplements in sports science. It works by topping up phosphocreatine stores in muscle, which regenerates ATP during short, intense efforts — sprinting, lifting, jumping. The 2017 position stand from the International Society of Sports Nutrition concluded that creatine monohydrate is the most effective ergogenic nutritional supplement available for increasing high-intensity exercise capacity and lean body mass during training, and that its long-term safety profile is well established. [Kreider et al., 2017]
Important distinction: Creatine improves performance in the activity itself — you can train harder, recover faster between sets, and gain strength more efficiently. It does not function as a stimulant or general “energy boost” for someone who feels tired at their desk. Newer research also suggests modest cognitive benefits, especially under sleep deprivation, but this is a smaller effect than the muscle benefit.
Typical dose: 3 to 5 grams per day of creatine monohydrate, taken any time of day. A loading phase (20 g/day for 5 to 7 days) saturates muscle faster but is not required. Mix with water or juice.
Safety: Decades of trials have found no consistent harm in healthy adults. The most common effect is a few pounds of weight gain from water held in muscle. People with kidney disease should consult a doctor first.
Caffeine
Caffeine is the most widely used psychoactive substance in the world, and the FDA notes that up to 400 mg per day — roughly four to five cups of coffee — is not generally associated with negative effects in healthy adults. [FDA, 2024] It works by blocking adenosine receptors in the brain, which reduces the sensation of tiredness and improves alertness, reaction time, and short-term focus.
Where caffeine helps: A quick mental lift before a meeting, sustained focus during the morning, or a 20- to 40-minute pre-workout window for endurance and strength performance. Lower doses (50 to 200 mg) generally work as well as higher ones for cognitive tasks, with fewer side effects.
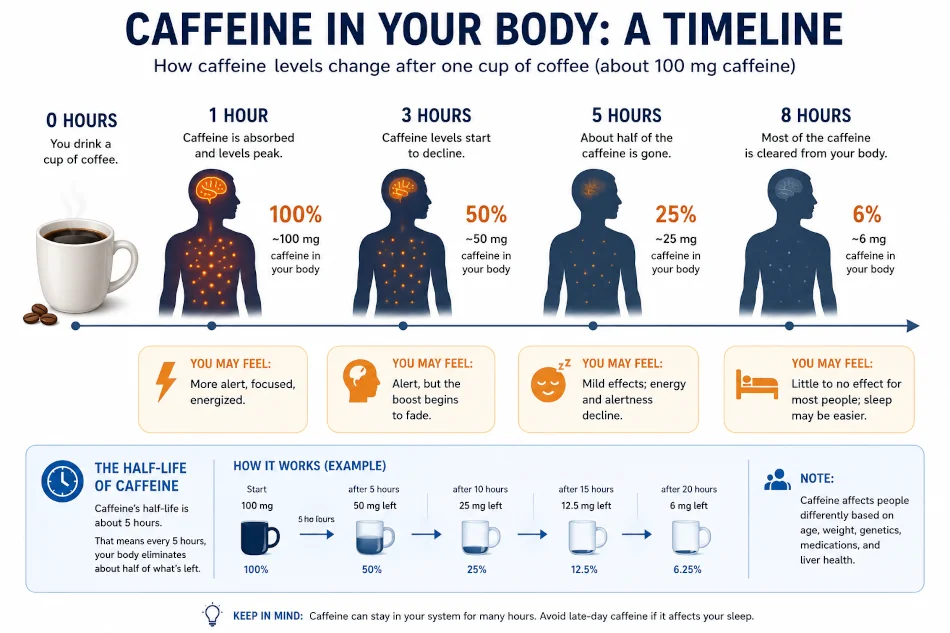
Where caffeine backfires: Past about 2 p.m. for most people — caffeine has a half-life of around 5 hours, so an afternoon coffee can still measurably impair sleep at bedtime, which then deepens next-day fatigue. Mayo Clinic also warns that pregnant women should keep intake under 200 mg per day, and people with anxiety, arrhythmias, GERD, or insomnia often do better on much less. [Mayo Clinic, 2024]
Powders and pills: Pure powdered caffeine is dangerous — a single teaspoon equals roughly 28 cups of coffee, and accidental overdose has been fatal. Avoid bulk powder; tablets in standard 100–200 mg doses are far safer. If you also want to understand how caffeine fits with other metabolic-support compounds, see our guide to herbs that speed up metabolism.
A Note on Energy Drinks and Multi-Ingredient Blends
Most commercial energy drinks combine caffeine with sugar, taurine, B vitamins, and proprietary herbal blends at undisclosed doses. The short-term lift comes almost entirely from caffeine and sugar. The B vitamins added to these drinks do not provide extra energy unless you were deficient to start with — your body excretes what it cannot use. Children, teenagers, pregnant women, and people with heart conditions should be especially cautious; the American Academy of Pediatrics recommends children and adolescents avoid energy drinks altogether.
Realistic Expectations: What Supplements Cannot Do
Even the best evidence-backed supplement is a small lever. None of them out-performs the basics:
- Consistent sleep schedule (same wake time, even on weekends).
- Daily movement — even 20 to 30 minutes of walking raises mitochondrial efficiency over time.
- Protein at every meal to steady blood sugar and reduce afternoon crashes.
- Limiting alcohol, which fragments sleep even at modest doses.
- Managing chronic stress — chronically elevated cortisol mimics fatigue and drives poor sleep.
Supplements work best as a targeted top-up when one of these foundations is already in place, or when bloodwork has identified a specific gap.
Who Should Be Especially Careful
Talk to a doctor or pharmacist before adding any of the supplements in this article if you:
- are pregnant, trying to conceive, or breastfeeding;
- take prescription medications, especially blood thinners (warfarin, apixaban), thyroid hormones, diabetes medications, blood-pressure drugs, lithium, MAO inhibitors, or chemotherapy;
- have kidney disease, liver disease, heart arrhythmias, or an autoimmune condition;
- have surgery scheduled within two weeks (several supplements affect bleeding and anesthesia);
- are giving the supplement to a child or teen — most supplements in this article are not appropriate for under-18s without medical guidance.
Many people assume “natural” means “safe to combine,” but real interactions are common. CoQ10 can blunt warfarin. Iron can block thyroid medication. Ashwagandha may push thyroid hormone levels higher in people who are already on replacement. Bring a list of every supplement to your next medical appointment, the same way you would for any prescription.
When Fatigue Needs a Doctor, Not a Supplement
Some symptoms are red flags that point to a medical problem no supplement will solve. Seek prompt care if your fatigue is accompanied by:
- unexplained weight loss or appetite loss;
- shortness of breath at rest or with light activity, chest pain, or palpitations;
- blood in stool or urine, very heavy or prolonged menstrual bleeding, or unusual bruising;
- persistent fever, night sweats, or swollen lymph nodes;
- new neurological symptoms — numbness, weakness, vision changes, confusion, memory loss;
- loud snoring with daytime sleepiness (possible sleep apnea);
- low mood, loss of interest, or thoughts of self-harm — fatigue is a common feature of depression, which is highly treatable.
Fatigue that has lasted more than six weeks despite reasonable sleep, diet, and stress management deserves a clinical workup — not another bottle.
| Health Disclaimer This article is for general educational and informational purposes only. It is not medical advice and is not a substitute for diagnosis or treatment by a qualified healthcare professional. Supplements can interact with medications and may not be appropriate for everyone, including people who are pregnant or breastfeeding, children, older adults, and anyone with a chronic medical condition. Talk to your doctor or pharmacist before starting a new supplement, especially if you are already on prescription medications, have a diagnosed condition, or notice persistent fatigue that does not improve with rest and a balanced diet. |
Frequently Asked Questions
What is the single best supplement for energy?
There is no universal best. The supplement most likely to help you is the one filling an actual gap. If a blood test shows you are low in iron, B12, or vitamin D, replacing that nutrient is far more powerful than any “energy formula.” If your bloodwork is normal, lifestyle changes will out-perform any pill.
How quickly do energy supplements work?
Caffeine works within 30 to 60 minutes. Iron, B12, and vitamin D — when correcting a true deficiency — usually take 2 to 8 weeks before energy meaningfully improves. CoQ10 and ashwagandha studies typically run 8 to 12 weeks before measurable effects appear. If you feel a dramatic boost within an hour from anything other than caffeine, you are likely feeling placebo or stimulant additives.
Can I take several of these together?
Sometimes, but not always. Iron and calcium block each other’s absorption. CoQ10 and warfarin interact. High-dose caffeine plus ashwagandha can produce conflicting effects (one stimulating, one calming). Ask a pharmacist to review your full list — they do this routinely and at no cost in most U.S. pharmacies.
Are food sources better than supplements?
For most nutrients, yes. Food provides cofactors and other compounds that improve absorption and usefulness — vitamin C with iron, fat with vitamin D, fiber and minerals together. Supplements are best thought of as a backup for situations where food alone cannot close the gap (vegan diets and B12, limited sun and vitamin D, heavy menstrual loss and iron).
Do energy supplements help with chronic fatigue syndrome or long COVID?
Evidence is limited and mixed. CoQ10 has the most supportive data for chronic fatigue–type symptoms. Stimulants and intense “energy formulas” can actually worsen post-exertional malaise in ME/CFS and long COVID. Anyone with these conditions should work with a clinician familiar with them rather than self-experiment.
References
1. Tsai I-C, Hsu C-W, Chang C-H, Tseng P-T, Chang K-V. Effectiveness of Coenzyme Q10 Supplementation for Reducing Fatigue: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in Pharmacology. 2022;13:883251. doi:10.3389/fphar.2022.883251. → View source
2. Kreider RB, Kalman DS, Antonio J, et al. International Society of Sports Nutrition position stand: safety and efficacy of creatine supplementation in exercise, sport, and medicine. Journal of the International Society of Sports Nutrition. 2017;14:18. doi:10.1186/s12970-017-0173-z. → View source
3. Kennedy DO. B Vitamins and the Brain: Mechanisms, Dose and Efficacy—A Review. Nutrients. 2016;8(2):68. doi:10.3390/nu8020068. → View source
4. Pérez-Gómez J, Villafaina S, Adsuar JC, Merellano-Navarro E, Collado-Mateo D. Effects of Ashwagandha (Withania somnifera) on VO2max: A Systematic Review and Meta-Analysis. Nutrients. 2020;12(4):1119. doi:10.3390/nu12041119. → View source
5. National Institutes of Health, Office of Dietary Supplements. Iron — Fact Sheet for Health Professionals. Updated 2023. → View source
6. National Institutes of Health, Office of Dietary Supplements. Vitamin B12 — Fact Sheet for Health Professionals. → View source
7. National Institutes of Health, Office of Dietary Supplements. Vitamin D — Fact Sheet for Health Professionals. → View source
8. Mayo Clinic. Iron deficiency anemia — Symptoms and causes. Reviewed 2025. → View source
9. Mayo Clinic. Caffeine: How much is too much? Reviewed 2024. → View source
10. U.S. Food and Drug Administration. Spilling the Beans: How Much Caffeine is Too Much? Updated 2023. → View source
11. National Center for Complementary and Integrative Health. Ashwagandha. Updated 2023. → View source
12. Harvard Health Publishing, Harvard Medical School. Best vitamins and minerals for energy. Updated 2024. → View source